Horne Hisani N, Phelan-Emrick Darcy F, Pollack Craig E, Markakis Diane, Wenzel Jennifer, Ahmed Saifuddin, Garza Mary A, Shapiro Gary R, Bone Lee R, Johnson Lawrence B, Ford Jean G
Cancer Prevention Fellowship Program, Division of Cancer Prevention, National Cancer Institute, National Institutes of Health, Rockville, MD, USA.
National Institutes of Health/NCI/DCEG/HREB, 9609 Medical Center Drive, Rm 7E234, MSC 7234, Bethesda, MD, 20892-7234, USA.
Cancer Causes Control. 2015 Feb;26(2):239-246. doi: 10.1007/s10552-014-0505-0. Epub 2014 Dec 17.
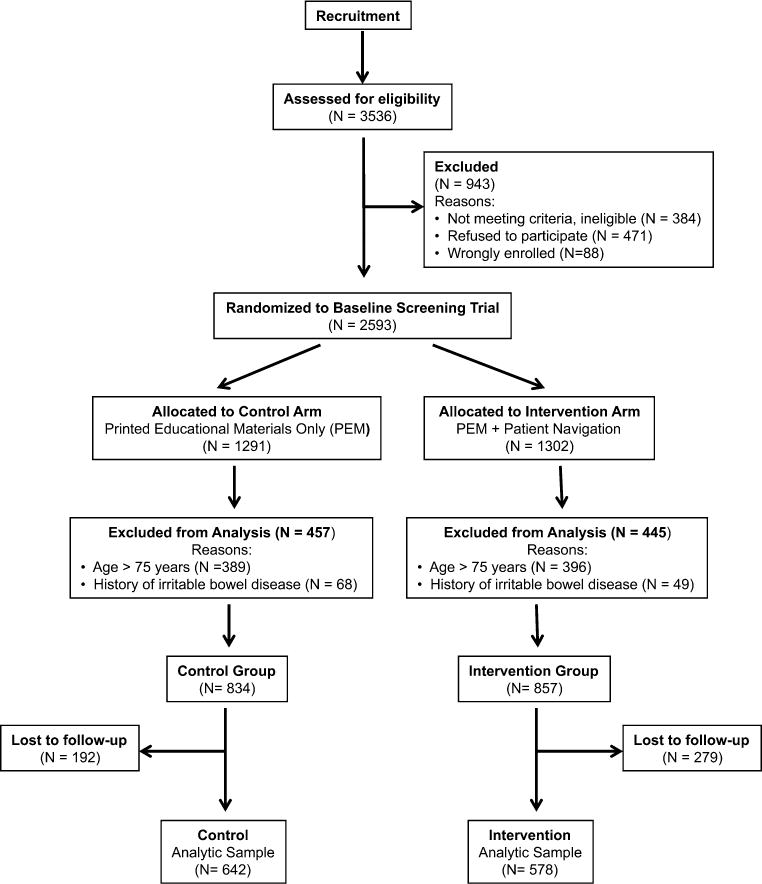
In recent years, colorectal cancer (CRC) screening rates have increased steadily in the USA, though racial and ethnic disparities persist. In a community-based randomized controlled trial, we investigated the effect of patient navigation on increasing CRC screening adherence among older African Americans.
Participants in the Cancer Prevention and Treatment Demonstration were randomized to either the control group, receiving only printed educational materials (PEM), or the intervention arm where they were assigned a patient navigator in addition to PEM. Navigators assisted participants with identifying and overcoming screening barriers. Logistic regression analyses were used to assess the effect of patient navigation on CRC screening adherence. Up-to-date with screening was defined as self-reported receipt of colonoscopy/sigmoidoscopy in the previous 10 years or fecal occult blood testing (FOBT) in the year prior to the exit interview.
Compared with controls, the intervention group was more likely to report being up-to-date with CRC screening at the exit interview (OR 1.55, 95 % CI 1.07-2.23), after adjusting for select demographics. When examining the screening modalities separately, the patient navigator increased screening for colonoscopy/sigmoidoscopy (OR 1.53, 95 % CI 1.07-2.19), but not FOBT screening. Analyses of moderation revealed stronger effects of navigation among participants 65-69 years and those with an adequate health literacy level.
In a population of older African Americans adults, patient navigation was effective in increasing the likelihood of CRC screening. However, more intensive navigation may be necessary for adults over 70 years and individuals with low literacy levels.
近年来,美国结直肠癌(CRC)筛查率稳步上升,尽管种族和族裔差异依然存在。在一项基于社区的随机对照试验中,我们研究了患者导航对提高老年非裔美国人CRC筛查依从性的影响。
癌症预防与治疗示范项目的参与者被随机分为对照组,仅接受印刷版教育材料(PEM),或干预组,除PEM外还为他们分配一名患者导航员。导航员协助参与者识别并克服筛查障碍。采用逻辑回归分析评估患者导航对CRC筛查依从性的影响。筛查最新情况定义为在过去10年中自我报告接受过结肠镜检查/乙状结肠镜检查,或在退出访谈前一年接受过粪便潜血试验(FOBT)。
在调整了选定的人口统计学因素后,与对照组相比,干预组在退出访谈时更有可能报告CRC筛查最新情况(比值比1.55,95%置信区间1.07 - 2.23)。当分别检查筛查方式时,患者导航员增加了结肠镜检查/乙状结肠镜检查的筛查率(比值比1.53,95%置信区间1.07 - 2.19),但未增加FOBT筛查率。调节分析显示,在65 - 69岁的参与者和健康素养水平足够的参与者中,导航的效果更强。
在老年非裔美国成年人中,患者导航有效地提高了CRC筛查的可能性。然而,对于70岁以上的成年人和低识字水平的个体,可能需要更密集的导航。