Ciacio Oriana, Voron Thibault, Pittau Gabriella, Lewin Maité, Vibert Eric, Adam René, Sa Cunha Antonio, Cherqui Daniel, Schielke Astrid, Soubrane Olivier, Scatton Olivier, Salloum Chady, Azoulay Daniel, Benoist Stéphane, Goyer Perrine, Vaillant Jean-Christophe, Hannoun Laurent, Boleslawski Emmanuel, Agostini Hélène, Samuel Didier, Castaing Denis
Centre Hépato-biliaire, Paul Brousse Hospital - APHP, 12-14 Avenue Paul Vaillant Couturier, 94800 Villejuif, France.
BMC Cancer. 2014 Dec 18;14:980. doi: 10.1186/1471-2407-14-980.
Malnutrition is an independent risk factor of postoperative morbidity and mortality and it's observed in 20 to 50% of surgical patients. Preoperative interventions to optimize the nutritional status, reduce postoperative complications and enteral nutrition has proven to be superior to the parenteral one. Moreover, regardless of the nutritional status of the patient, surgery impairs the immunological response, thus increasing the risk of postoperative sepsis. Immunonutrition has been developed to improve the immunometabolic host response in perioperative period and it has been proven to reduce significantly postoperative infectious complications and length of hospital stay in patients undergoing elective gastrointestinal surgery for tumors. We hypothesize that a preoperative oral immunonutrition (ORAL IMPACT®) can reduce postoperative morbidity in liver resection for cancer.
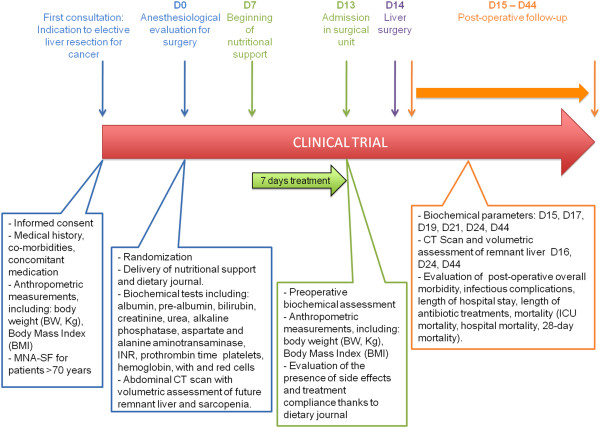
METHODS/DESIGN: Prospective multicenter randomized placebo-controlled double-blind phase IV trial with two parallel treatment groups receiving either study product (ORAL IMPACT®) or control supplement (isocaloric isonitrogenous supplement--IMPACT CONTROL®) for 7 days before liver resection for cancer. A total of 400 patients will be enrolled. Patients will be stratified according to the type of hepatectomy, the presence of chronic liver disease and the investigator center. The main end-point is to evaluate in intention-to-treat analysis the overall 30-day morbidity. Secondary end-points are to assess the 30-day infectious and non-infectious morbidity, length of antibiotic treatment and hospital stay, modifications on total food intake, compliance to treatment, side-effects of immunonutrition, impact on liver regeneration and sarcopenia, and to perform a medico-economic analysis.
The overall morbidity rate after liver resection is 22% to 42%. Infectious post-operative complications (12% to 23%) increase the length of hospital stay and costs and are responsible for a quarter of 30-day mortality. Various methods have been advocated to decrease the rate of postoperative complications but there is no evidence to support or refute the use of any treatment and further trials are required. The effects of preoperative oral immunonutrition in non-cirrhotic patients undergoing liver resection for cancer are unknown. The present trial is designed to evaluate whether the administration of a short-term preoperative oral immunonutrition can reduce postoperative morbidity in non-cirrhotic patients undergoing liver resection for cancer.
Clinicaltrial.gov: NCT02041871.
营养不良是术后发病和死亡的独立危险因素,在20%至50%的外科手术患者中可见。优化营养状况、减少术后并发症的术前干预措施以及肠内营养已被证明优于肠外营养。此外,无论患者的营养状况如何,手术都会损害免疫反应,从而增加术后败血症的风险。免疫营养已被开发用于改善围手术期宿主的免疫代谢反应,并且已被证明可显著降低接受择期肿瘤胃肠手术患者的术后感染并发症和住院时间。我们假设术前口服免疫营养(ORAL IMPACT®)可降低肝癌肝切除术后的发病率。
方法/设计:前瞻性多中心随机安慰剂对照双盲IV期试验,有两个平行治疗组,在肝癌肝切除术前7天分别接受研究产品(ORAL IMPACT®)或对照补充剂(等热量等氮补充剂——IMPACT CONTROL®)。总共将招募400名患者。患者将根据肝切除术的类型、慢性肝病的存在情况和研究中心进行分层。主要终点是在意向性分析中评估30天总体发病率。次要终点是评估30天感染性和非感染性发病率、抗生素治疗时间和住院时间、总食物摄入量的变化、治疗依从性、免疫营养的副作用、对肝再生和肌肉减少症的影响,并进行药物经济学分析。
肝切除术后的总体发病率为22%至42%。术后感染并发症(12%至23%)会增加住院时间和费用,并且是30天死亡率的四分之一原因。已经提倡了各种方法来降低术后并发症的发生率,但没有证据支持或反驳任何治疗方法的使用,还需要进一步的试验。术前口服免疫营养对非肝硬化肝癌肝切除患者的影响尚不清楚。本试验旨在评估短期术前口服免疫营养的给药是否能降低非肝硬化肝癌肝切除患者的术后发病率。
Clinicaltrial.gov:NCT02041871。