Lin Shang-Yi, Chen Tun-Chieh, Lu Po-Liang, Lin Chun-Yu, Lin Wei-Ru, Yang Yi-Hsin, Chen Yen-Hsu
Kaohsiung Municipal Ta-Tung Hospital, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan.
School of Medicine, Graduate Institute of Medicine, Sepsis Research Center, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan.
BMC Infect Dis. 2014 Dec 19;14:705. doi: 10.1186/s12879-014-0705-y.
It is debated whether interferon-based therapy (IBT) would affect the incidence of active tuberculosis (TB) among hepatitis C virus (HCV) infected patients. Although some case reports have demonstrated a possible association, the results are currently inconclusive. Therefore, we conducted a nation-wide population study to investigate the incidence of active TB in HCV infected patients receiving IBT in Taiwan.
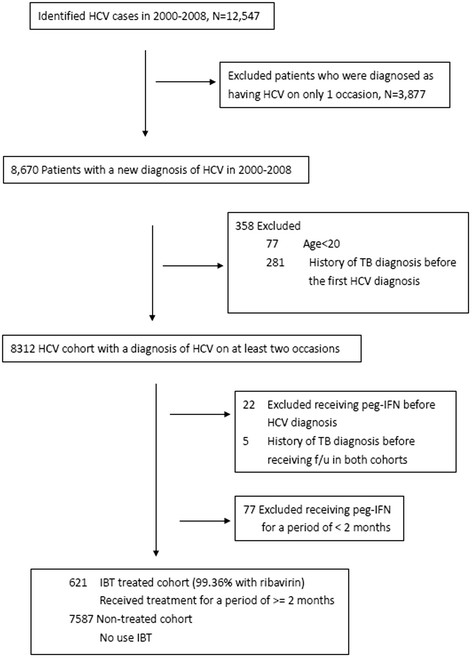
This 9-year cohort study was based on the Longitudinal Health Insurance Database 2000 (LHID 2000) consisting of 1,000,000 beneficiaries randomly selected from all Taiwan National Health Insurance enrollees in 2000 ( >23.7 million). This insurance program covers all citizens in Taiwan. We conducted a retrospective cohort study that identified subjects with HCV infection. IBTs were defined as regimens that included interferon α, peginterferon α2a and peginterferon α2b for at least 2 months. Among them, 621 subjects received IBT, and 2,460 age- and gender-matched subjects were enrolled for analysis. The Cox proportional hazards models were used to estimate the hazard ratio (HR) for active TB, and associated confidence intervals (CIs), comparing IBT cohort and untreated cohort. The endpoint in this study was whether an enrolled subject had a new diagnosis of active TB.
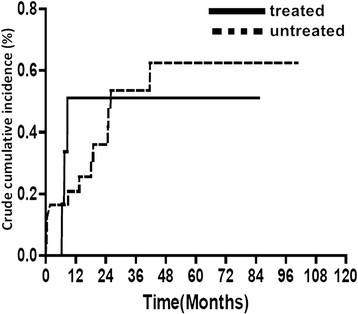
During the 9-year enrollment period, the treated and untreated cohorts were followed for a mean (± SD) duration of 6.97 ± 0.02 years and 8.21 ± 0.01 years, respectively. The cumulative incidence rate of active TB during this study period was 0.150 and 0.151 per 100 person-years in the IBT treated and untreated cohorts, respectively. There was no significant difference in the incidence of active TB in either cohort during a 1-year follow-up (Adjusted Hazard Ratio (AHR): 2.81, 95% Confidence Interval (95% CI): 0.61-12.98) or the long-term follow-up (AHR: 1.02, 95% CI: 0.28-3.78). The Cox proportional hazards model demonstrated that IBT was not a risk factor for active TB . The only risk factor for active TB was the occurrence of hepatic encephalopathy.
Our results showed that IBT is associated with increased hazard of active TB in HCV infected patients in 1-year follow-up; however, the effect sizes were not statistically significant.
基于干扰素的治疗(IBT)是否会影响丙型肝炎病毒(HCV)感染患者中活动性结核病(TB)的发病率仍存在争议。尽管一些病例报告显示可能存在关联,但目前结果尚无定论。因此,我们进行了一项全国性的人群研究,以调查台湾接受IBT的HCV感染患者中活动性TB的发病率。
这项为期9年的队列研究基于2000年纵向健康保险数据库(LHID 2000),该数据库由2000年从所有台湾国民健康保险参保者(超过2370万)中随机选取的100万受益人组成。该保险计划覆盖台湾所有公民。我们进行了一项回顾性队列研究,确定HCV感染的受试者。IBT被定义为包括干扰素α、聚乙二醇干扰素α2a和聚乙二醇干扰素α2b至少2个月的治疗方案。其中,621名受试者接受了IBT,2460名年龄和性别匹配的受试者被纳入分析。使用Cox比例风险模型估计活动性TB的风险比(HR)以及相关的置信区间(CI),比较IBT队列和未治疗队列。本研究的终点是登记的受试者是否有新诊断的活动性TB。
在9年的入组期间,治疗组和未治疗组的平均(±标准差)随访时间分别为6.97±0.02年和8.21±0.01年。在本研究期间,IBT治疗组和未治疗组中活动性TB的累积发病率分别为每100人年0.150和0.151。在1年随访期间(调整后风险比(AHR):2.81,95%置信区间(95%CI):0.61 - 12.98)或长期随访期间(AHR:1.02,95%CI:0.28 - 3.78),两组中活动性TB的发病率均无显著差异。Cox比例风险模型表明,IBT不是活动性TB的危险因素。活动性TB的唯一危险因素是肝性脑病的发生。
我们的结果表明,在1年随访中,IBT与HCV感染患者活动性TB的风险增加相关;然而,效应大小无统计学意义。