Division of Gastroenterology, Department of Internal Medicine, Buddhist Tzu Chi General Hospital, Taipei Branch, Taipei, Taiwan.
PLoS One. 2013 Jul 23;8(7):e70458. doi: 10.1371/journal.pone.0070458. Print 2013.
Interferon-based therapy (IBT) has been the standard of care for hepatitis C virus (HCV) infection. However, conflicting results exist regarding the effects of IBT on risk of developing hepatocellular carcinoma (HCC) and cirrhosis-associated complications, and most included highly selected patients.
This 8-year cohort study was based on the Longitudinal Health Insurance Database 2000 (LHID 2000) consisting of 1,000,000 beneficiaries randomly selected from all Taiwan National Health Insurance enrollees in 2000 (>23.7 million). Patients with newly detected HCV infections (n=11,264) were classified based on treatment and clinical outcomes. IBTs were defined as regimens that included interferon- alfa, pegylated interferon- alfa -2a, or pegylated interferon- alfa -2b for at least 3 months. The Cox proportional hazards models were used to estimate the hazard ratio (HR) and associated confidence interval (CI) of HCC and cirrhosis-associated complications for IBT.
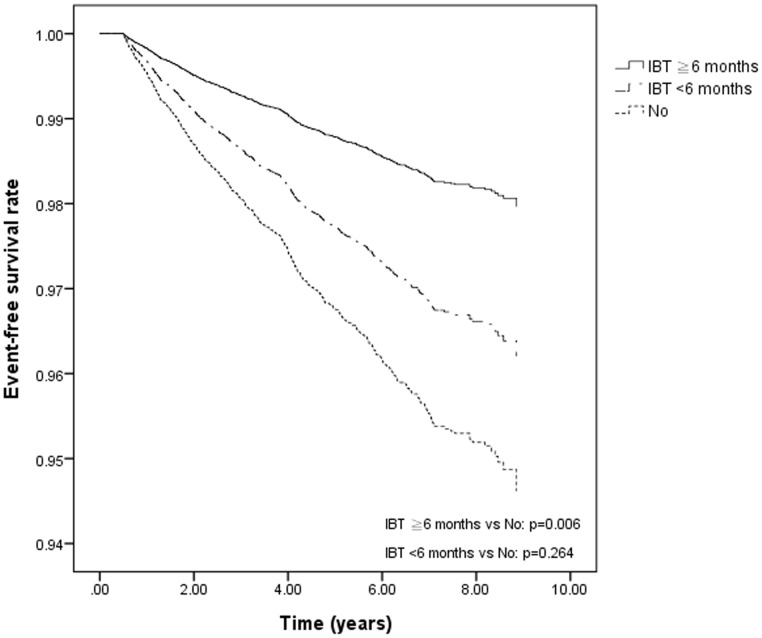
The 8-year incidence rate for HCC was 3.9% among patients who received IBT and 5.6% among those who did not. The HCC-free survival rate was significantly higher among patients receiving IBT during the 8-year period than their counterpart (adjusted HR, 0.50; 95% CI, 0.31-0.81; P= .004). Similarly, the event-free survival rates for esophageal variceal bleeding (adjusted HR, 0.45; 95% CI, 0.22-0.91; P= .026), hepatic encephalopathy (adjusted HR, 0.38; 95% CI, 0.21-0.69; P= .001), ascites (adjusted HR, 0.28; 95% CI, 0.14-0.57; P<.001), and cirrhosis (adjusted HR, 0.63; 95% CI, 0.44-0.91; P= .013) were significantly higher among patients who received IBT than those who did not, after adjustment for associated factors.
Treatment with interferon may reduce the 8-year risk of HCC and cirrhosis-associated complications in patients with chronic HCV infection.
基于干扰素的治疗(IBT)一直是丙型肝炎病毒(HCV)感染的标准治疗方法。然而,关于 IBT 对肝细胞癌(HCC)和肝硬化相关并发症风险的影响,存在相互矛盾的结果,而且大多数研究纳入的都是高度选择的患者。
这项 8 年的队列研究基于 2000 年纵向健康保险数据库(LHID 2000),该数据库由 2000 年从所有台湾全民健康保险参保者中随机抽取的 100 万名受益人的数据组成(>2370 万人)。根据治疗和临床结局,将新诊断为 HCV 感染的患者(n=11264)进行分类。IBT 定义为至少接受干扰素-α、聚乙二醇化干扰素-α-2a 或聚乙二醇化干扰素-α-2b 治疗 3 个月以上的方案。采用 Cox 比例风险模型估计 IBT 治疗 HCC 和肝硬化相关并发症的风险比(HR)和相关置信区间(CI)。
接受 IBT 治疗的患者在 8 年内 HCC 的发生率为 3.9%,未接受 IBT 治疗的患者为 5.6%。在 8 年期间,接受 IBT 治疗的患者 HCC 无进展生存率显著高于对照组(调整后的 HR,0.50;95%CI,0.31-0.81;P=0.004)。同样,接受 IBT 治疗的患者食管静脉曲张出血(调整后的 HR,0.45;95%CI,0.22-0.91;P=0.026)、肝性脑病(调整后的 HR,0.38;95%CI,0.21-0.69;P=0.001)、腹水(调整后的 HR,0.28;95%CI,0.14-0.57;P<.001)和肝硬化(调整后的 HR,0.63;95%CI,0.44-0.91;P=0.013)的无事件生存率也显著高于未接受 IBT 治疗的患者,调整了相关因素后。
慢性 HCV 感染患者接受干扰素治疗可能会降低 8 年内 HCC 和肝硬化相关并发症的风险。