Feng L, Wu J T, Liu X, Yang P, Tsang T K, Jiang H, Wu P, Yang J, Fang V J, Qin Y, Lau E H, Li M, Zheng J, Peng Z, Xie Y, Wang Q, Li Z, Leung G M, Gao G F, Yu H, Cowling B J
Division of Infectious Disease, Key Laboratory of Surveillance and Early-warning on Infectious Disease, Chinese Center for Disease Control and Prevention (China CDC), Beijing, China.
Euro Surveill. 2014 Dec 11;19(49):20984. doi: 10.2807/1560-7917.es2014.19.49.20984.
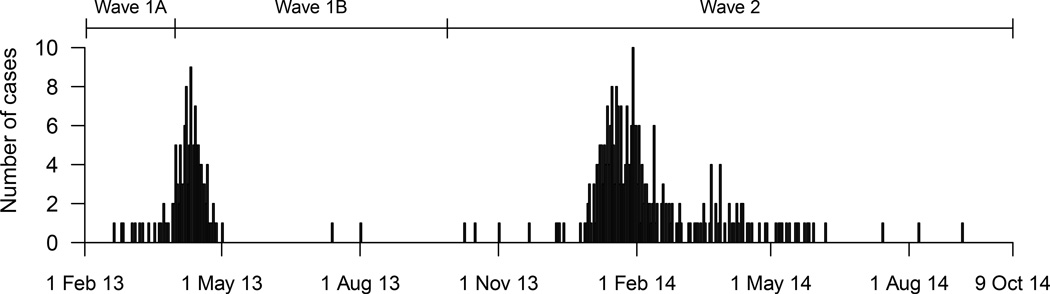
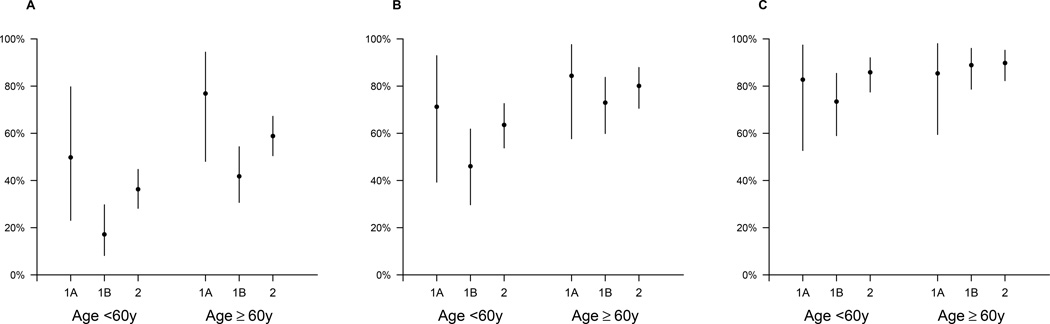
Assessing the severity of emerging infections is challenging because of potential biases in case ascertainment. The first human case of infection with influenza A(H7N9) virus was identified in China in March 2013; since then, the virus has caused two epidemic waves in the country. There were 134 laboratory-confirmed cases detected in the first epidemic wave from January to September 2013. In the second epidemic wave of human infections with avian influenza A(H7N9) virus in China from October 2013 to October 2014, we estimated that the risk of death among hospitalised cases of infection with influenza A(H7N9) virus was 48% (95% credibility interval: 42-54%), slightly higher than the corresponding risk in the first wave. Age-specific risks of death among hospitalised cases were also significantly higher in the second wave. Using data on symptomatic cases identified through national sentinel influenza-like illness surveillance, we estimated that the risk of death among symptomatic cases of infection with influenza A(H7N9) virus was 0.10% (95% credibility interval: 0.029-3.6%), which was similar to previous estimates for the first epidemic wave of human infections with influenza A(H7N9) virus in 2013. An increase in the risk of death among hospitalised cases in the second wave could be real because of changes in the virus, because of seasonal changes in host susceptibility to severe infection, or because of variation in treatment practices between hospitals, while the increase could be artefactual because of changes in ascertainment of cases in different areas at different times.
由于病例确诊过程中存在潜在偏差,评估新出现感染的严重程度具有挑战性。2013年3月在中国发现了首例人感染甲型H7N9流感病毒病例;自那时以来,该病毒在中国引发了两波疫情。在2013年1月至9月的第一波疫情中,共检测到134例实验室确诊病例。在中国2013年10月至2014年10月的第二波人感染甲型H7N9流感病毒疫情中,我们估计甲型H7N9流感病毒感染住院病例的死亡风险为48%(95%可信区间:42%-54%),略高于第一波疫情中的相应风险。住院病例中按年龄划分的死亡风险在第二波疫情中也显著更高。利用通过全国流感样病例哨点监测确定的有症状病例的数据,我们估计甲型H7N9流感病毒有症状感染病例的死亡风险为0.10%(95%可信区间:0.029%-3.6%),这与之前对2013年第一波人感染甲型H7N9流感病毒疫情的估计相似。第二波疫情中住院病例死亡风险的增加可能是真实的,原因可能是病毒发生了变化、宿主对严重感染的易感性出现季节性变化,或者是不同医院治疗方法存在差异,而这种增加也可能是由于不同地区在不同时间病例确诊情况的变化导致的人为现象。