Claussen Peter Andreas, Abdelnoor Michael, Kvakkestad Kristin M, Eritsland Jan, Halvorsen Sigrun
Department of Cardiology, Oslo University Hospital, Ullevaal, Norway ; Faculty of Medicine, University of Oslo, Oslo, Norway.
Centre of Clinical Research: Unit of Epidemiology and Biostatistics, Oslo University Hospital, Ullevaal, Norway.
Vasc Health Risk Manag. 2014 Dec 9;10:683-9. doi: 10.2147/VHRM.S72764. eCollection 2014.
Elderly patients with ST-segment elevation myocardial infarction (STEMI) are at high risk for complications and early mortality; still, they are underrepresented in clinical trials and observational studies. We studied the risk profiles at presentation and early mortality in elderly (≥80 years) versus younger (<80 years) STEMI patients.
This was a prospective cohort study.
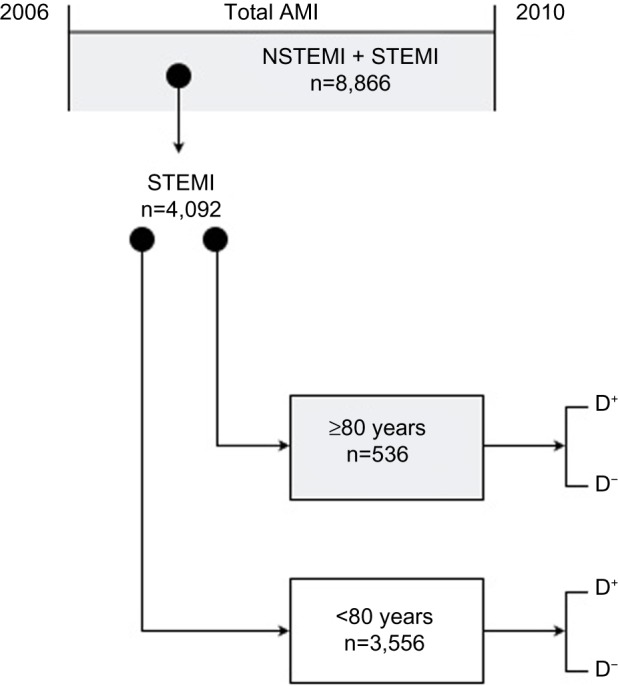
The study population comprised 4,092 consecutive STEMI patients admitted to Oslo University Hospital, Ulleval from 2006 to 2010. Baseline characteristics at admission were recorded, as well as in-hospital mortality. Etiologic strategy was used in the analyses.
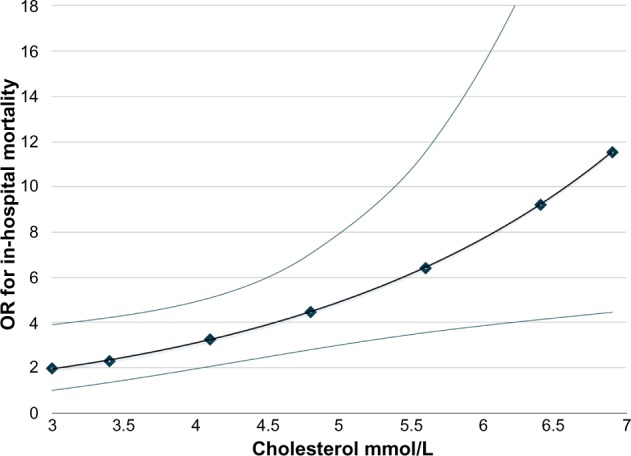
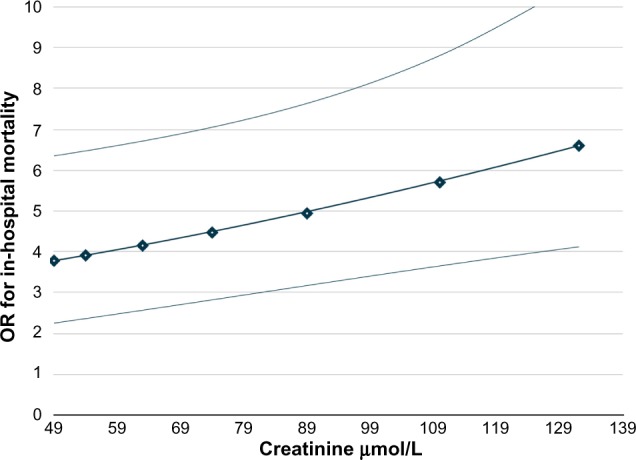
Patients ≥80 years of age (n=536) were more likely to be women and have prior myocardial infarction, angina, and stroke, but were less likely to be current smokers. The crude in-hospital mortality was 16.2% in patients aged 80 years and older versus 3.5% in those younger than 80 years. The adjusted odds ratio for mortality in patients aged 80 years and older versus those younger than 80 years increased with increasing levels of serum creatinine and total cholesterol. In patients with low levels of serum creatinine and total cholesterol, the odds ratio was 3.01 (95% confidence interval, 1.86-4.93; P=0.0001); increasing to 11.72 (95% confidence interval, 5.26-26.3; P=0.001) in patients with high levels.
High levels of serum cholesterol and creatinine were important risk factors for early mortality in elderly patients. Depending on the levels of cholesterol and creatinine, in-hospital mortality in patients aged 80 years and older varied from a threefold to an almost twelvefold risk compared with younger patients.
ST 段抬高型心肌梗死(STEMI)老年患者并发症和早期死亡率风险较高;然而,他们在临床试验和观察性研究中的代表性不足。我们研究了老年(≥80 岁)与年轻(<80 岁)STEMI 患者就诊时的风险特征和早期死亡率。
这是一项前瞻性队列研究。
研究人群包括 2006 年至 2010 年连续入住奥斯陆大学医院乌勒瓦尔分院的 4092 例 STEMI 患者。记录入院时的基线特征以及院内死亡率。分析采用病因学策略。
≥80 岁的患者(n = 536)更可能为女性,并有既往心肌梗死、心绞痛和中风史,但当前吸烟者较少。80 岁及以上患者的粗院内死亡率为 16.2%,而 80 岁以下患者为 3.5%。80 岁及以上患者与 80 岁以下患者相比,调整后的死亡比值比随血清肌酐和总胆固醇水平升高而增加。在血清肌酐和总胆固醇水平较低的患者中,比值比为 3.01(95%置信区间,1.86 - 4.93;P = 0.0001);在高水平患者中增至 11.72(95%置信区间,5.26 - 26.3;P = 0.001)。
血清胆固醇和肌酐水平升高是老年患者早期死亡的重要危险因素。根据胆固醇和肌酐水平,80 岁及以上患者的院内死亡率与年轻患者相比,风险从三倍到近十二倍不等。