Lauretti Gabriela Rocha, Veloso Fabricio S, Kitayama Antonio T, Mattos Anita Leocadia
Department of Biomechanics, Medicine and Rehabilitation of Locomotor Members, Discipline of Anesthesia and Pain Management, School of Medicine of Ribeirão Preto, University of São Paulo, Ribeirão Preto, São Paulo, Brazil.
Department of Anesthesia, School of Medicine of Ribeirão Preto, University of São Paulo, Ribeirão Preto, São Paulo, Brazil.
J Res Med Sci. 2014 Sep;19(9):801-6.
Opioids are considered mainstream for combined spinal-epidural anesthesia, but frequently limited by adverse effects. The aim of this study was to examine whether low-dose spinal neostigmine, epidural dexamethasone or their combination enhances analgesia from spinal bupivacaine without adverse effects.
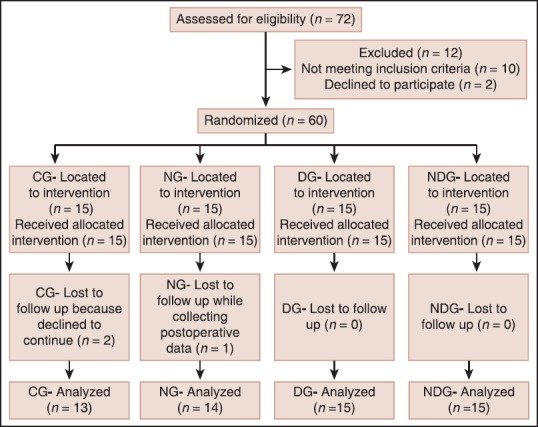
A total of 60 patients undergoing orthopedic surgery were randomized to one of four groups and evaluated for 24-h after surgery for analgesia (time to first rescue analgesic) and rescue analgesic consumption. Patients received 15 mg bupivacaine plus the test drug intrathecally (saline or 1 microgram (μg) neostigmine). The epidural test drug was either saline or 10 mg dexamethasone. The Control group (CG) received spinal and epidural saline. The Neostigmine group (NG), spinal neostigmine and epidural saline; the Dexamethasone group (DG), spinal saline and epidural dexamethasone; and the Neostigmine-dexamethasone group (NDG), spinal neostigmine and epidural dexamethasone.
The CG (282 ± 163 min) and NG (524 ± 142 min) were similar in their times to first rescue analgesic and analgesic consumption. The time to first rescue analgesic was longer for the DG (966 ± 397 min) compared with CG and NG (P < 0.0002), and the DG had less ketoprofen consumption and lower overall visual analogue scale-pain sores compared with CG and NG (P < 0.0005). Addition of 1 mg-neostigmine (NDG) resulted in longer time to rescue analgesic (1205 ± 303 min; P < 0.02) and lower ketoprofen consumption (P < 0.05) compared to DG. Sporadic cases of vesical catheterization and emesis were observed, however adverse effects were similar among groups.
Spinal 1 microgram (μg) neostigmine further enhanced analgesia from spinal bupivacaine combined with epidural dexamethasone, without increasing the incidence of adverse effects.
阿片类药物被认为是腰麻-硬膜外联合麻醉的主流用药,但常受不良反应限制。本研究旨在探讨低剂量脊髓新斯的明、硬膜外注射地塞米松或二者联合使用能否增强布比卡因腰麻的镇痛效果且无不良反应。
总共60例接受骨科手术的患者被随机分为四组之一,并在术后24小时评估镇痛情况(首次使用补救镇痛药的时间)和补救镇痛药的消耗量。患者鞘内注射15mg布比卡因加试验药物(生理盐水或1微克新斯的明)。硬膜外试验药物为生理盐水或10mg地塞米松。对照组(CG)接受腰麻和硬膜外注射生理盐水。新斯的明组(NG),鞘内注射新斯的明和硬膜外注射生理盐水;地塞米松组(DG),鞘内注射生理盐水和硬膜外注射地塞米松;新斯的明-地塞米松组(NDG),鞘内注射新斯的明和硬膜外注射地塞米松。
CG组(282±163分钟)和NG组(524±142分钟)首次使用补救镇痛药的时间和镇痛药消耗量相似。与CG组和NG组相比,DG组首次使用补救镇痛药的时间更长(966±397分钟)(P<0.0002),且与CG组和NG组相比,DG组酮洛芬消耗量更少,总体视觉模拟评分-疼痛评分更低(P<0.0005)。与DG组相比,添加1mg新斯的明(NDG组)导致补救镇痛药使用时间更长(1205±303分钟;P<0.02),酮洛芬消耗量更低(P<0.05)。观察到偶发膀胱导尿和呕吐病例,然而各组间不良反应相似。
鞘内注射1微克新斯的明可进一步增强布比卡因腰麻联合硬膜外地塞米松的镇痛效果,且不增加不良反应发生率。