van den Bosch Harrie C M, Westenberg Jos J M, Setz-Pels Wikke, Wondergem John, Wolterbeek Ron, Duijm Lucien E M, Teijink Joep A W, de Roos Albert
Department of Radiology, Catharina Hospital, Michelangelolaan 2, Eindhoven, The Netherlands.
J Cardiovasc Magn Reson. 2015 Jan 20;17(1):2. doi: 10.1186/s12968-014-0095-8.
Vascular disease expression in one location may not be representative for disease severity in other vascular territories, however, strong correlation between disease expression and severity within the same vascular segment may be expected. Therefore, we hypothesized that aortic stiffening is more strongly associated with disease expression in a vascular territory directly linked to that aortic segment rather than in a more remote segment. We prospectively compared the association between aortic wall stiffness, expressed by pulse wave velocity (PWV), sampled in the distal aorta, with the severity of peripheral arterial occlusive disease (PAOD) as compared to atherosclerotic markers sampled in remote vascular territories such as PWV in the proximal aorta and the normalized wall index (NWI), representing the vessel wall thickness, of the left common carotid artery.
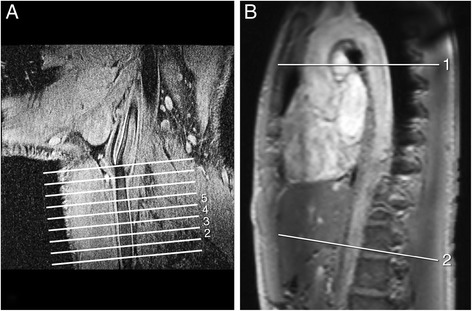
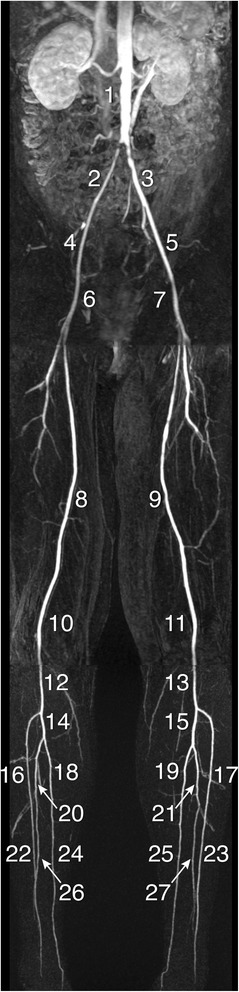
Forty-two patients (23 men; mean age 64±10 years) underwent velocity-encoded cardiovascular magnetic resonance (CMR) in the proximal and distal aorta, whole-body contrast-enhanced MR angiography (CE-MRA) and carotid vessel wall imaging with black-blood CMR in the work-up for PAOD. Strength of associations between aortic stiffness, carotid NWI and peripheral vascular stenosis grade were assessed and evaluated with multiple linear regression.
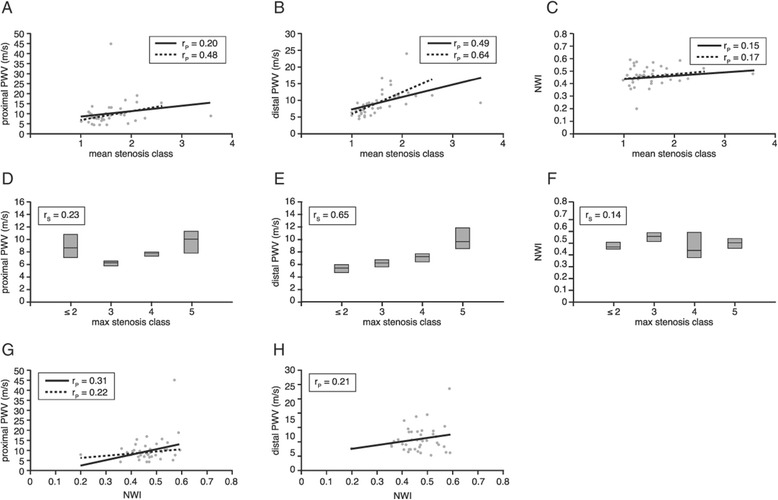
Stenosis severity correlated well with PWV in the distal aorta (Pearson rP=0.64, p<0.001, Spearman rS=0.65, p<0.001) but to a lesser extent with PWV in the proximal aorta (rP=0.48, p=0.002, rS=0.22, p=0.18). Carotid NWI was not associated with peripheral stenosis severity (rP=0.17, p=0.28, rS=0.14, p=0.37) nor with PWV in the proximal aorta (rP=0.22, p=0.17) nor in the distal aorta (rP=0.21, p=0.18). Correlation between stenosis severity and distal aortic PWV remained statistically significant after correction for age and gender.
Distal aortic wall stiffness is more directly related to peripheral arterial stenosis severity than markers from more remote vascular territories such as proximal aortic wall stiffness or carotid arterial wall thickness. Site-specific evaluation of vascular disease may be required for full vascular risk estimation.
血管疾病在一个部位的表现可能无法代表其他血管区域的疾病严重程度,然而,同一血管节段内疾病表现与严重程度之间可能存在强相关性。因此,我们假设主动脉僵硬度与直接连接该主动脉节段的血管区域的疾病表现关联更强,而非与更远端节段的关联更强。我们前瞻性地比较了在远端主动脉采样的以脉搏波速度(PWV)表示的主动脉壁僵硬度与外周动脉闭塞性疾病(PAOD)严重程度之间的关联,并与在近端主动脉的PWV以及代表左颈总动脉血管壁厚度的标准化壁指数(NWI)等远端血管区域采样的动脉粥样硬化标志物进行了比较。
42例患者(23例男性;平均年龄64±10岁)在PAOD检查过程中接受了近端和远端主动脉的速度编码心血管磁共振成像(CMR)、全身对比增强磁共振血管造影(CE-MRA)以及颈动脉血管壁的黑血CMR成像。通过多元线性回归评估和评价主动脉僵硬度、颈动脉NWI与外周血管狭窄分级之间的关联强度。
狭窄严重程度与远端主动脉的PWV相关性良好(Pearson rP = 0.64,p < 0.001,Spearman rS = 0.65,p < 0.001),但与近端主动脉的PWV相关性较弱(rP = 0.48,p = 0.002,rS = 0.22,p = 0.18)。颈动脉NWI与外周狭窄严重程度无关(rP = 0.17,p = 0.28,rS = 0.14,p = 0.37),与近端主动脉的PWV无关(rP = 0.22,p = 0.17),与远端主动脉的PWV也无关(rP = 0.21,p = 0.18)。在校正年龄和性别后,狭窄严重程度与远端主动脉PWV之间的相关性仍具有统计学意义。
远端主动脉壁僵硬度比来自更远端血管区域的标志物(如近端主动脉壁僵硬度或颈动脉壁厚度)与外周动脉狭窄严重程度的关系更直接。全面评估血管风险可能需要对血管疾病进行部位特异性评估。