King M-F, Noakes C J, Sleigh P A
School of Civil Engineering, Pathogen Control Engineering Institute, University of Leeds, Leeds, UK.
Indoor Air. 2015 Dec;25(6):694-707. doi: 10.1111/ina.12186. Epub 2015 Mar 4.
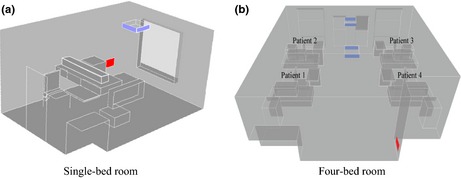
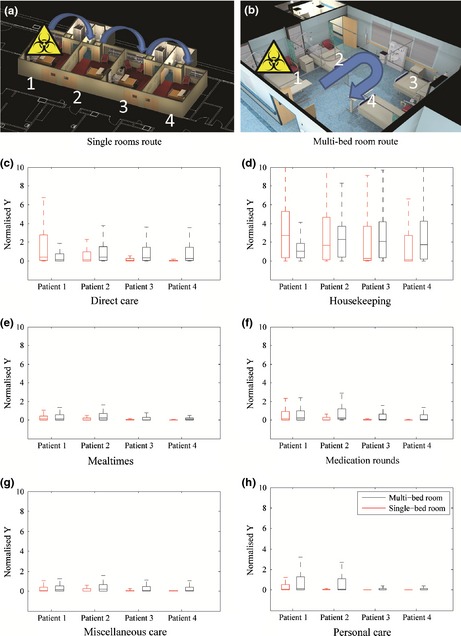
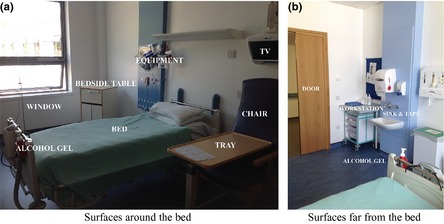
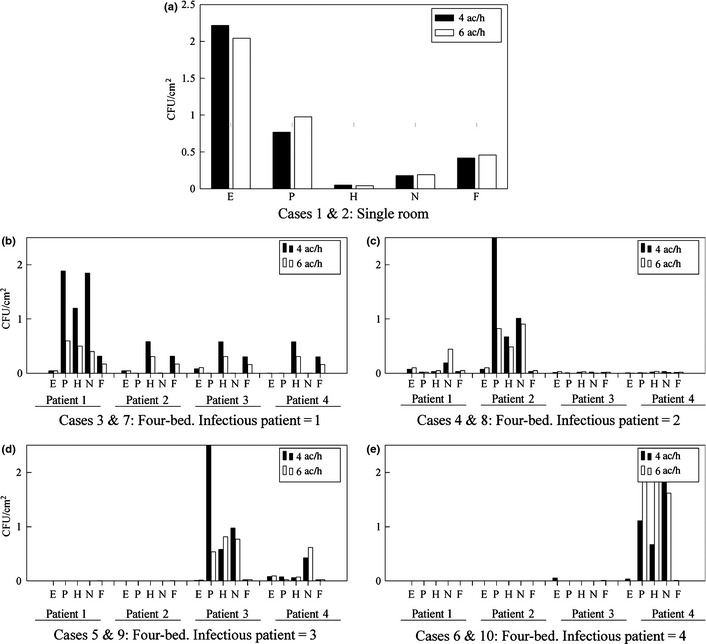
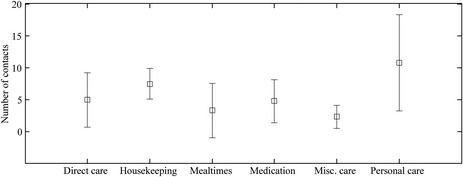
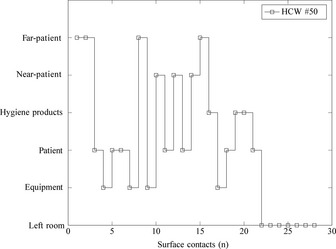
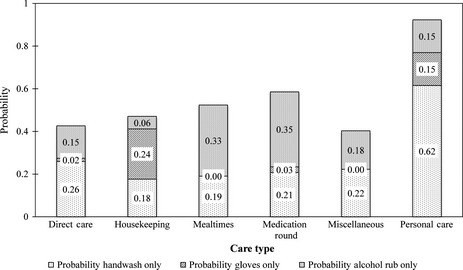
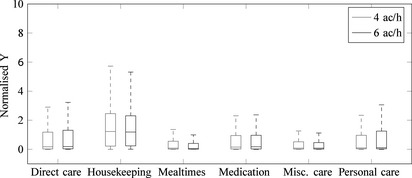
Aerial dispersion of pathogens is recognized as a potential transmission route for hospital acquired infections; however, little is known about the link between healthcare worker (HCW) contacts' with contaminated surfaces, the transmission of infections and hospital room design. We combine computational fluid dynamics (CFD) simulations of bioaerosol deposition with a validated probabilistic HCW-surface contact model to estimate the relative quantity of pathogens accrued on hands during six types of care procedures in two room types. Results demonstrate that care type is most influential (P < 0.001), followed by the number of surface contacts (P < 0.001) and the distribution of surface pathogens (P = 0.05). Highest hand contamination was predicted during Personal care despite the highest levels of hand hygiene. Ventilation rates of 6 ac/h vs. 4 ac/h showed only minor reductions in predicted hand colonization. Pathogens accrued on hands decreased monotonically after patient care in single rooms due to the physical barrier of bioaerosol transmission between rooms and subsequent hand sanitation. Conversely, contamination was predicted to increase during contact with patients in four-bed rooms due to spatial spread of pathogens. Location of the infectious patient with respect to ventilation played a key role in determining pathogen loadings (P = 0.05).
We present the first quantitative model predicting the surface contacts by HCW and the subsequent accretion of pathogenic material as they perform standard patient care. This model indicates that single rooms may significantly reduce the risk of cross-contamination due to indirect infection transmission. Not all care types pose the same risks to patients, and housekeeping performed by HCWs may be an important contribution in the transmission of pathogens between patients. Ventilation rates and positioning of infectious patients within four-bed rooms can mitigate the accretion of pathogens, whereby reducing the risk of missed hand hygiene opportunities. The model provides a tool to quantitatively evaluate the influence of hospital room design on infection risk.
病原体的空气传播被认为是医院获得性感染的一种潜在传播途径;然而,对于医护人员(HCW)与受污染表面的接触、感染传播与病房设计之间的联系,我们却知之甚少。我们将生物气溶胶沉积的计算流体动力学(CFD)模拟与经过验证的概率性医护人员-表面接触模型相结合,以估算在两种病房类型中进行六种护理程序时手上累积的病原体相对数量。结果表明,护理类型的影响最大(P < 0.001),其次是表面接触次数(P < 0.001)和表面病原体分布(P = 0.05)。尽管手部卫生水平最高,但在个人护理期间预计手部污染程度最高。每小时换气6次与每小时换气4次相比,预计手部定植仅略有减少。由于病房之间生物气溶胶传播的物理屏障以及随后的手部清洁,单人病房中患者护理后手上累积的病原体单调减少。相反,预计在四人间与患者接触期间污染会增加,这是由于病原体的空间传播。感染患者相对于通风口的位置在确定病原体负荷方面起着关键作用(P = 0.05)。
我们提出了第一个定量模型,用于预测医护人员在进行标准患者护理时与表面的接触以及随后致病物质的累积。该模型表明,单人病房可能会显著降低因间接感染传播导致交叉污染的风险。并非所有护理类型对患者构成的风险都相同,医护人员进行的清洁工作可能是病原体在患者之间传播的一个重要因素。四人间的通风率和感染患者的位置可以减轻病原体的累积,从而降低错过手部卫生机会的风险。该模型提供了一种工具,用于定量评估病房设计对感染风险的影响。