Schulkes Karlijn J G, Van den Elzen Mignon T, Hack Erik C, Otten Henderikus G, Bruijnzeel-Koomen Carla A F M, Knulst André C
Department of Dermatology and Allergology, University Medical Center Utrecht (G02.124), PO Box 85.500, Utrecht, 3508 GA The Netherlands.
Laboratory of Translational Immunology, University Medical Center Utrecht, Utrecht, the Netherlands.
Clin Transl Allergy. 2015 Feb 4;5(1):5. doi: 10.1186/s13601-015-0049-8. eCollection 2015.
Non-hereditary angioedema (non-HAE) is characterized by local swelling due to self-limiting, subcutaneous or submucosal extravasation of fluid, and can be divided into three subtypes. These subtypes are believed to have different pathophysiological backgrounds and are referred to in recent guidelines as bradykinin-mediated (e.g. caused by angiotensin-converting-enzyme-inhibitors), mast cell-mediated (e.g. angioedema with wheals) or idiopathic (cause unknown). Bradykinin-mediated subtypes are more closely related to hereditary angioedema than the other forms. Because clinical features of these non-HAE subtypes have not been studied in detail, we have looked at the clinical characteristics of symptoms and potential differences in clinical presentation of bradykinin-mediated and mast cell-mediated angioedema (AE) subtypes.
A questionnaire was sent to patients presenting with AE at our tertiary outpatient clinic to document clinical characteristics, potential triggers and location of AE. The severity of AE attacks was analysed using visual analogue scales (VAS).
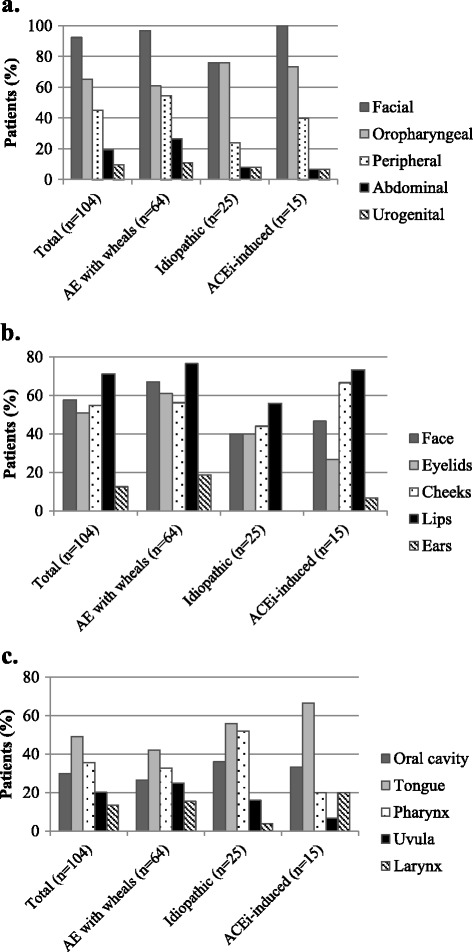
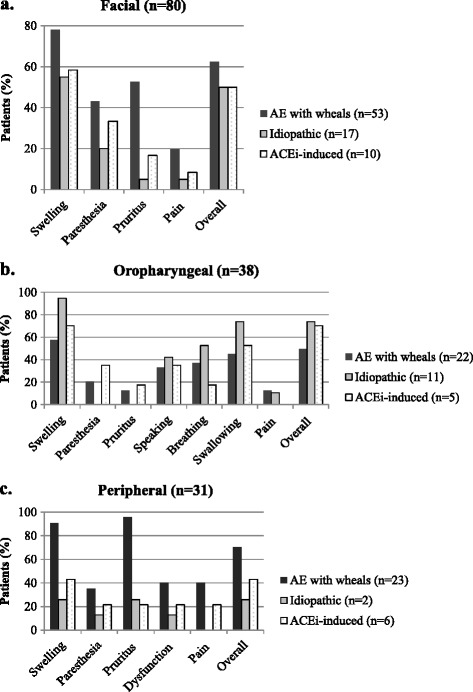
The questionnaire was returned by 106 patients, of which 104 were included in the analysis. AE with wheals, idiopathic AE, and drug-associated AE occurred in 64 (62%), 25 (24%) and 15 patients (14%) respectively. Most patients (62%) reported prodromal symptoms while 63% reported multiple locations for an attack. Face and oropharynx were the main locations of AE attacks of any subtype while swelling was the symptom most frequently reported as severe. Overall severity of the last attack was indicated as severe by 68% of the patients. There were no differences between the subgroups.
This similarity in clinical presentation raises the possibility that ACEi-induced, mast cell-mediated and idiopathic AE share common pathways.
非遗传性血管性水肿(non-HAE)的特征是由于液体的自限性皮下或粘膜下渗出导致局部肿胀,可分为三种亚型。这些亚型被认为具有不同的病理生理背景,在最近的指南中被称为缓激肽介导型(例如由血管紧张素转换酶抑制剂引起)、肥大细胞介导型(例如伴有风团的血管性水肿)或特发性(病因不明)。缓激肽介导型亚型与遗传性血管性水肿的关系比其他形式更为密切。由于尚未对这些非HAE亚型的临床特征进行详细研究,我们研究了缓激肽介导型和肥大细胞介导型血管性水肿(AE)亚型的症状临床特征及临床表现的潜在差异。
向我们三级门诊就诊的AE患者发送问卷,以记录AE的临床特征、潜在诱因和发病部位。使用视觉模拟量表(VAS)分析AE发作的严重程度。
106例患者回复了问卷,其中104例纳入分析。伴有风团的AE、特发性AE和药物相关性AE分别发生在64例(62%)、25例(24%)和15例(14%)患者中。大多数患者(62%)报告有前驱症状,63%报告发作部位有多处。面部和口咽是任何亚型AE发作的主要部位,而肿胀是最常报告为严重的症状。68%的患者表示最后一次发作的总体严重程度为严重。各亚组之间无差异。
临床表现的这种相似性增加了ACEi诱导型、肥大细胞介导型和特发性AE具有共同途径的可能性。