Williams Jessica N, Rai Ashish, Lipscomb Joseph, Koff Jean L, Nastoupil Loretta J, Flowers Christopher R
Emory University School of Medicine, Atlanta, Georgia.
Department of Health Policy and Management, Rollins School of Public Health, Emory University, Atlanta, Georgia.
Cancer. 2015 Jun 1;121(11):1800-8. doi: 10.1002/cncr.29290. Epub 2015 Feb 11.
Although the combination of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) is considered standard therapy for diffuse large B-cell lymphoma (DLBCL), patterns of use and the impact of R-CHOP on survival in patients aged >80 years are less clear.
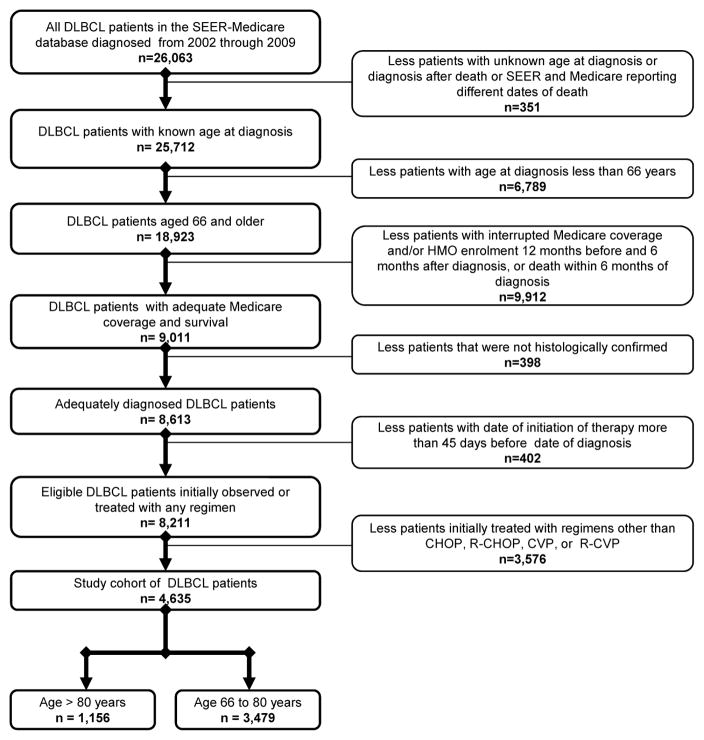
The Surveillance, Epidemiology, and End Results (SEER)-Medicare database was used to characterize presentation, treatment, and survival patterns in patients with DLBCL who were diagnosed between 2002 and 2009. Chi-square tests compared characteristics and initial treatments among patients with DLBCL who were aged >80 years and ≤80 years. Multivariable logistic regression models examined factors associated with treatment selection in patients aged >80 years; standard and propensity score-adjusted multivariable Cox proportional hazards models examined relationships between treatment regimen, treatment duration, and survival.
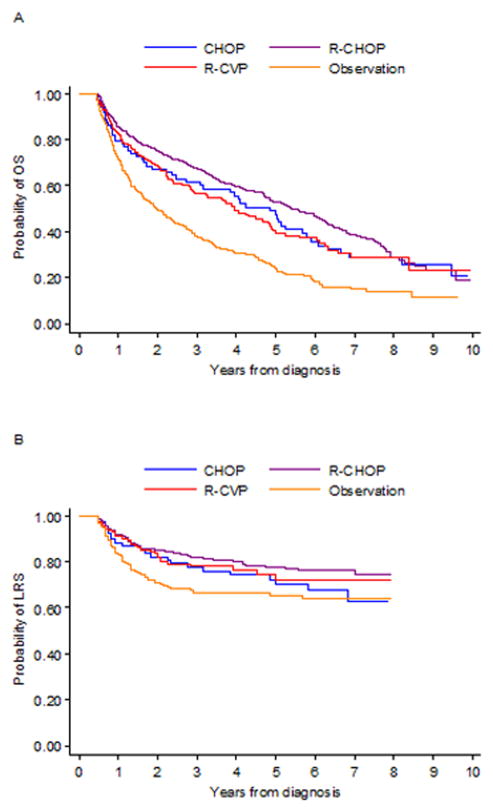
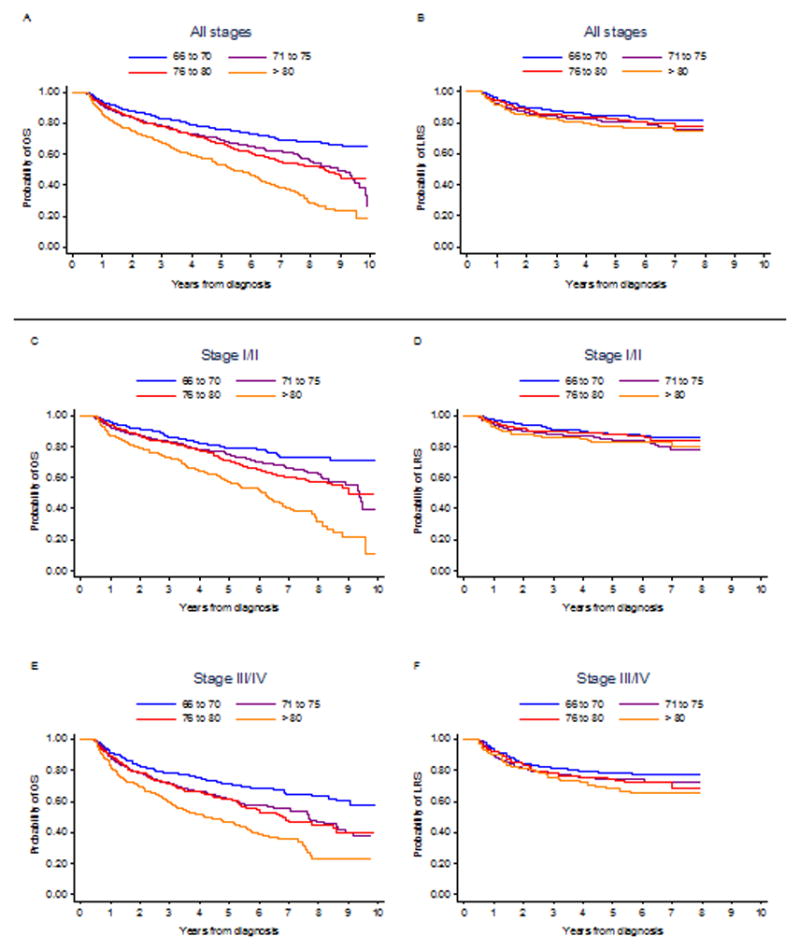
Among 4635 patients with DLBCL, 1156 (25%) were aged >80 years. Patients aged >80 years were less likely to receive R-CHOP and more likely to be observed or receive the combination of rituximab, cyclophosphamide, vincristine, and prednisone (P<.0001 for both). Marital status, stage of disease, disease site, performance status, radiotherapy, and growth factor support were associated with initial R-CHOP in patients aged >80 years. In propensity score-matched multivariable Cox proportional hazards models examining relationships between treatment regimen and survival, R-CHOP was the only regimen found to be associated with improved overall survival (hazard ratio, 0.45; 95% confidence interval, 0.33-0.62) and lymphoma-related survival (hazard ratio, 0.58; 95% confidence interval, 0.38-0.88).
Although patients with DLBCL who were aged >80 years were less likely to receive R-CHOP, this regimen conferred the longest survival and should be considered for this population. Further studies are needed to characterize the impact of treatment of DLBCL on quality of life among patients in this age group.
尽管利妥昔单抗、环磷酰胺、阿霉素、长春新碱和泼尼松联合方案(R-CHOP)被认为是弥漫性大B细胞淋巴瘤(DLBCL)的标准治疗方案,但对于80岁以上患者的使用模式以及R-CHOP对其生存的影响尚不清楚。
利用监测、流行病学和最终结果(SEER)-医疗保险数据库来描述2002年至2009年期间诊断为DLBCL的患者的临床表现、治疗和生存模式。卡方检验比较了年龄>80岁和≤80岁的DLBCL患者的特征和初始治疗情况。多变量逻辑回归模型研究了80岁以上患者治疗选择的相关因素;标准和倾向评分调整的多变量Cox比例风险模型研究了治疗方案、治疗持续时间与生存之间的关系。
在4635例DLBCL患者中,1156例(25%)年龄>80岁。80岁以上的患者接受R-CHOP治疗的可能性较小,更有可能接受观察或接受利妥昔单抗、环磷酰胺、长春新碱和泼尼松联合治疗(两者P均<0.0001)。婚姻状况、疾病分期、疾病部位、体能状态、放疗和生长因子支持与80岁以上患者初始接受R-CHOP治疗有关。在倾向评分匹配的多变量Cox比例风险模型中研究治疗方案与生存之间的关系时,发现R-CHOP是唯一与总生存改善相关的方案(风险比,0.45;95%置信区间,0.33-0.62)以及与淋巴瘤相关生存相关的方案(风险比,0.58;95%置信区间,0.38-0.88)。
尽管年龄>80岁的DLBCL患者接受R-CHOP治疗的可能性较小,但该方案带来的生存时间最长,应考虑用于该人群。需要进一步研究来描述DLBCL治疗对该年龄组患者生活质量的影响。