Massie A B, Chow E K H, Wickliffe C E, Luo X, Gentry S E, Mulligan D C, Segev D L
Department of Surgery, Johns Hopkins University School of Medicine, Baltimore, MD; Department of Epidemiology, Johns Hopkins School of Public Health, Baltimore, MD.
Am J Transplant. 2015 Mar;15(3):659-67. doi: 10.1111/ajt.13099.
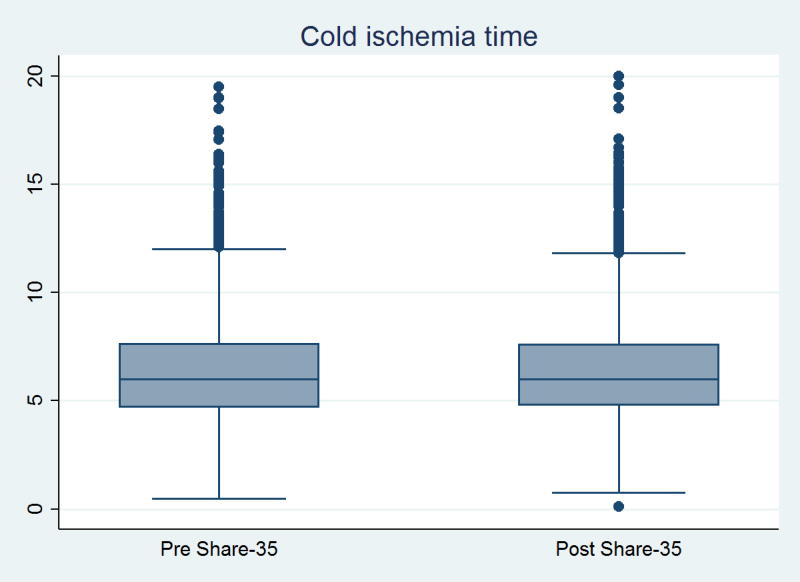
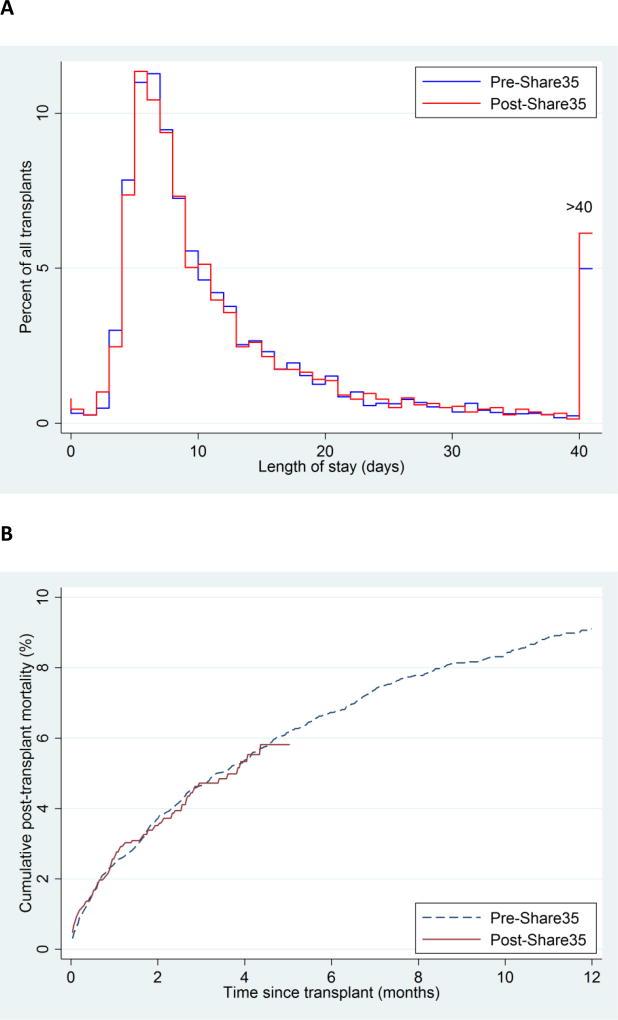
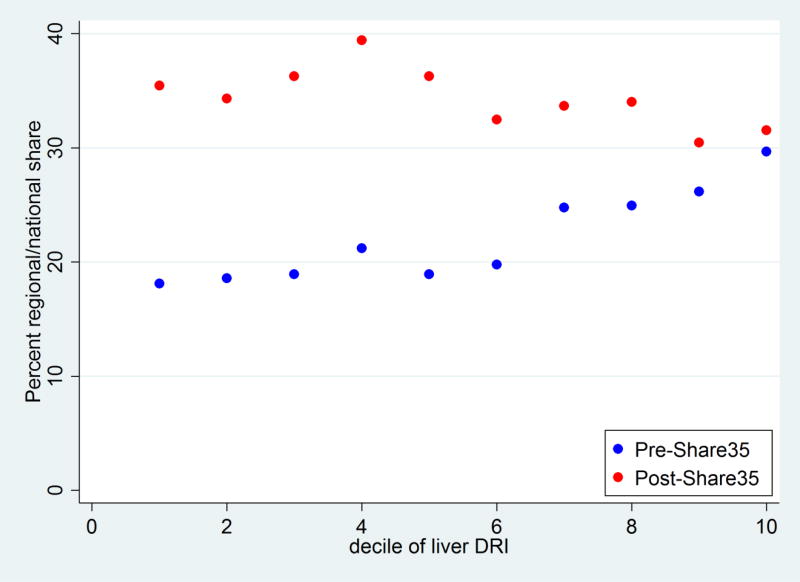
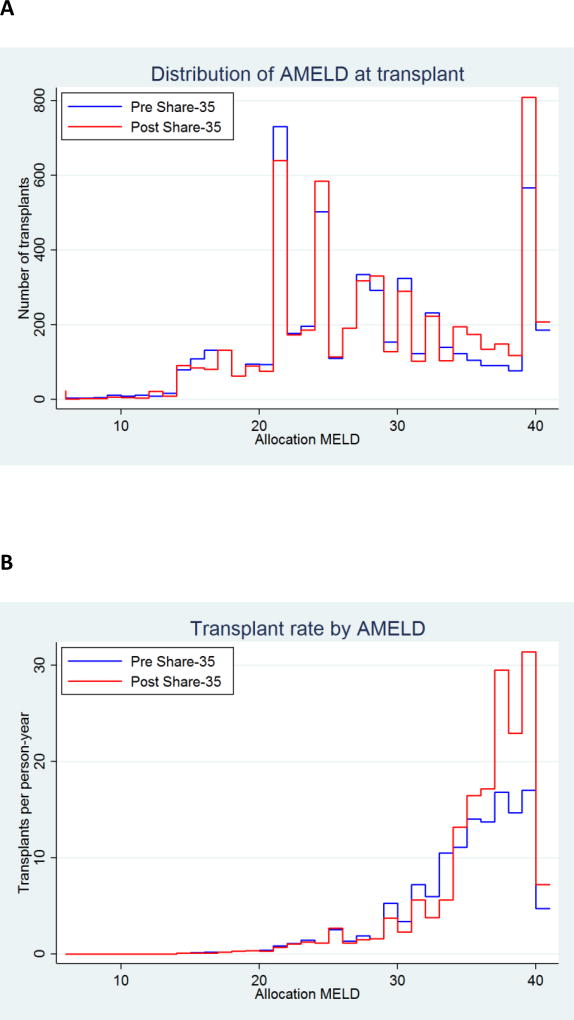
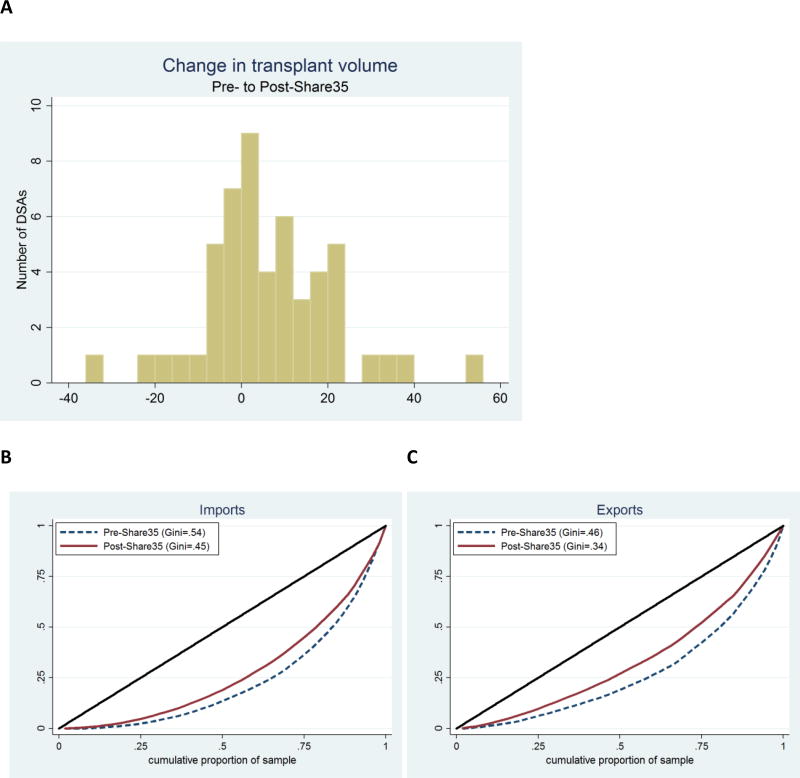
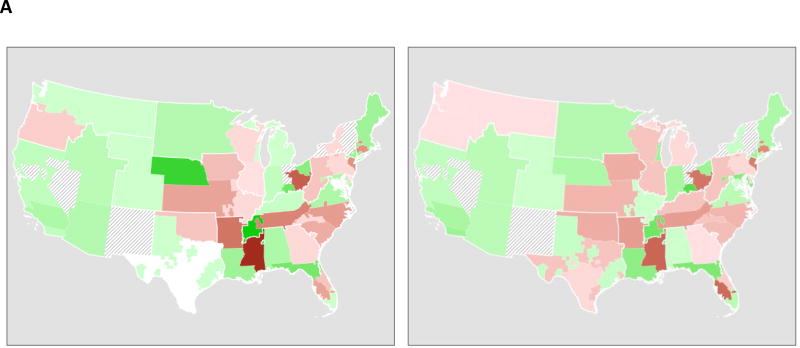
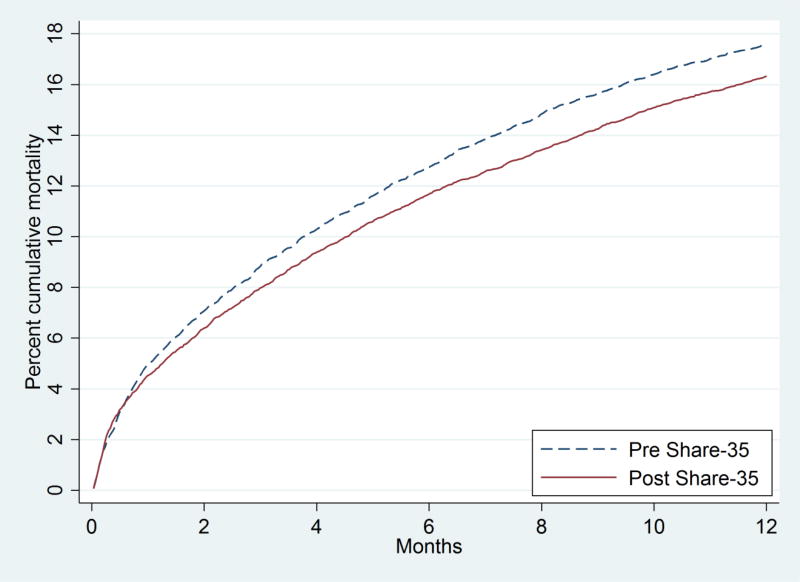
In June 2013, a change to the liver waitlist priority algorithm was implemented. Under Share 35, regional candidates with MELD ≥ 35 receive higher priority than local candidates with MELD < 35. We compared liver distribution and mortality in the first 12 months of Share 35 to an equivalent time period before. Under Share 35, new listings with MELD ≥ 35 increased slightly from 752 (9.2% of listings) to 820 (9.7%, p = 0.3), but the proportion of deceased-donor liver transplants (DDLTs) allocated to recipients with MELD ≥ 35 increased from 23.1% to 30.1% (p < 0.001). The proportion of regional shares increased from 18.9% to 30.4% (p < 0.001). Sharing of exports was less clustered among a handful of centers (Gini coefficient decreased from 0.49 to 0.34), but there was no evidence of change in CIT (p = 0.8). Total adult DDLT volume increased from 4133 to 4369, and adjusted odds of discard decreased by 14% (p = 0.03). Waitlist mortality decreased by 30% among patients with baseline MELD > 30 (SHR = 0.70, p < 0.001) with no change for patients with lower baseline MELD (p = 0.9). Posttransplant length-of-stay (p = 0.2) and posttransplant mortality (p = 0.9) remained unchanged. In the first 12 months, Share 35 was associated with more transplants, fewer discards, and lower waitlist mortality, but not at the expense of CIT or early posttransplant outcomes.
2013年6月,肝脏等待名单优先算法发生了一项改变。在“共享35”政策下,终末期肝病模型(MELD)评分≥35的地区候选人比MELD评分<35的本地候选人获得更高的优先级。我们将“共享35”政策实施的前12个月内肝脏分配情况及死亡率与之前的同等时间段进行了比较。在“共享35”政策下,MELD评分≥35的新登记人数从752人(占登记人数的9.2%)略有增加至8