Carballo David, Delhumeau Cécile, Carballo Sebastian, Bähler Caroline, Radovanovic Dragona, Hirschel Bernard, Clerc Olivier, Bernasconi Enos, Fasel Dominique, Schmid Patrick, Cusini Alexia, Fehr Jan, Erne Paul, Keller Pierre-Fréderic, Ledergerber Bruno, Calmy Alexandra
Department of Cardiology, University Hospital, Geneva, Switzerland.
HIV Metabolic Clinic, University Hospital, Geneva, Switzerland.
AIDS Res Ther. 2015 Feb 22;12:4. doi: 10.1186/s12981-015-0045-z. eCollection 2015.
HIV infection may be associated with an increased recurrence rate of myocardial infarction. Our aim was to determine whether HIV infection is a risk factor for worse outcomes in patients with coronaray artery disease.
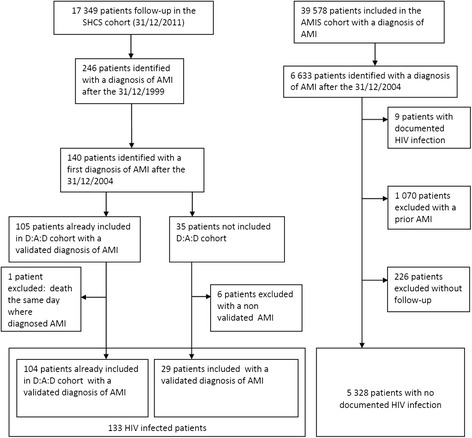
We compared data aggregated from two ongoing cohorts: (i) the Acute Myocardial Infarction in Switzerland (AMIS) registry, which includes patients with acute myocardial infarction (AMI), and (ii) the Swiss HIV Cohort Study (SHCS), a prospective registry of HIV-positive (HIV+) patients. We included all patients who survived an incident AMI occurring on or after 1st January 2005. Our primary outcome measure was all-cause mortality at one year; secondary outcomes included AMI recurrence and cardiovascular-related hospitalisations. Comparisons used Cox and logistic regression analyses, respectively.
There were 133 HIV+, (SHCS) and 5,328 HIV-negative [HIV-] (AMIS) individuals with incident AMI. In the SHCS and AMIS registries, patients were predominantly male (72% and 85% male, respectively), with a median age of 51 years (interquartile range [IQR] 46-57) and 64 years (IQR 55-74), respectively. Nearly all (90%) of HIV+ individuals were on successful antiretroviral therapy. During the first year of follow-up, 5 (3.6%) HIV+ and 135 (2.5%) HIV- individuals died. At one year, HIV+ status after adjustment for age, sex, calendar year of AMI, smoking status, hypertension and diabetes was associated with a higher risk of death (HR 4.42, 95% CI 1.73-11.27). There were no significant differences in recurrent AMIs (4 [3.0%] HIV+ and 146 [3.0%] HIV- individuals, OR 1.16, 95% CI 0.41-3.27) or in hospitalization rates (OR 0.68 [95% CI 0.42-1.11]).
HIV infection was associated with a significantly increased risk of all-cause mortality one year after incident AMI.
HIV感染可能与心肌梗死复发率增加有关。我们的目的是确定HIV感染是否是冠状动脉疾病患者预后较差的危险因素。
我们比较了两个正在进行的队列汇总的数据:(i)瑞士急性心肌梗死(AMIS)登记处,其中包括急性心肌梗死(AMI)患者,以及(ii)瑞士HIV队列研究(SHCS),这是一个HIV阳性(HIV+)患者的前瞻性登记处。我们纳入了所有在2005年1月1日或之后发生的首次AMI中存活下来的患者。我们的主要结局指标是一年时的全因死亡率;次要结局包括AMI复发和心血管相关住院。比较分别使用Cox和逻辑回归分析。
有133名HIV+(SHCS)和5328名HIV阴性[HIV-](AMIS)个体发生首次AMI。在SHCS和AMIS登记处,患者主要为男性(分别为72%和85%为男性),中位年龄分别为51岁(四分位间距[IQR]46 - 57)和64岁(IQR 55 - 74)。几乎所有(90%)的HIV+个体都接受了成功的抗逆转录病毒治疗。在随访的第一年,5名(3.6%)HIV+个体和135名(2.5%)HIV-个体死亡。在调整年龄、性别、AMI的日历年、吸烟状况、高血压和糖尿病后,HIV+状态与更高的死亡风险相关(风险比4.42,95%置信区间1.73 - 11.27)。复发性AMI(4名[3.0%]HIV+个体和146名[3.0%]HIV-个体,比值比1.16,95%置信区间0.41 - 3.27)或住院率(比值比0.68[95%置信区间0.42 - 1.11])没有显著差异。
HIV感染与首次AMI后一年时全因死亡率显著增加相关。