Kontopantelis Evangelos, Springate David A, Ashworth Mark, Webb Roger T, Buchan Iain E, Doran Tim
Centre for Health Informatics, Institute of Population Health, University of Manchester, Manchester, UK NIHR School for Primary Care Research, Centre for Primary Care, Institute of Population Health, University of Manchester
NIHR School for Primary Care Research, Centre for Primary Care, Institute of Population Health, University of Manchester Centre for Biostatistics, Institute of Population Health, University of Manchester.
BMJ. 2015 Mar 2;350:h904. doi: 10.1136/bmj.h904.
To quantify the relationship between a national primary care pay-for-performance programme, the UK's Quality and Outcomes Framework (QOF), and all-cause and cause-specific premature mortality linked closely with conditions included in the framework.
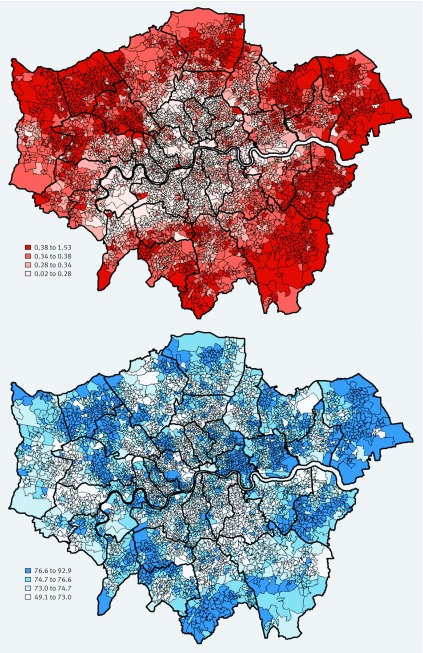
Longitudinal spatial study, at the level of the "lower layer super output area" (LSOA).
32482 LSOAs (neighbourhoods of 1500 people on average), covering the whole population of England (approximately 53.5 million), from 2007 to 2012.
8647 English general practices participating in the QOF for at least one year of the study period, including over 99% of patients registered with primary care.
National pay-for-performance programme incentivising performance on over 100 quality-of-care indicators.
All-cause and cause-specific mortality rates for six chronic conditions: diabetes, heart failure, hypertension, ischaemic heart disease, stroke, and chronic kidney disease. We used multiple linear regressions to investigate the relationship between spatially estimated recorded quality of care and mortality.
All-cause and cause-specific mortality rates declined over the study period. Higher mortality was associated with greater area deprivation, urban location, and higher proportion of a non-white population. In general, there was no significant relationship between practice performance on quality indicators included in the QOF and all-cause or cause-specific mortality rates in the practice locality.
Higher reported achievement of activities incentivised under a major, nationwide pay-for-performance programme did not seem to result in reduced incidence of premature death in the population.
量化一项全国性初级医疗绩效付费计划(英国的质量与结果框架,即QOF)与框架中所包含疾病密切相关的全因及特定病因过早死亡率之间的关系。
在“低层超级输出区”(LSOA)层面进行的纵向空间研究。
2007年至2012年期间,涵盖英格兰全体人口(约5350万)的32482个LSOA(平均每个社区1500人)。
8647家参与QOF至少一年研究期的英国全科医疗诊所,包括超过99%在初级医疗注册的患者。
全国性绩效付费计划,激励在100多项医疗质量指标上的表现。
六种慢性病(糖尿病、心力衰竭、高血压、缺血性心脏病、中风和慢性肾病)的全因及特定病因死亡率。我们使用多元线性回归来研究空间估计的记录医疗质量与死亡率之间的关系。
在研究期间,全因及特定病因死亡率均有所下降。较高的死亡率与更大程度的地区贫困、城市位置以及非白人人口的较高比例相关。总体而言,QOF中包含的质量指标方面的诊所表现与诊所所在地区的全因或特定病因死亡率之间没有显著关系。
在一项主要的全国性绩效付费计划下,较高的报告活动达成率似乎并未导致人群过早死亡发生率的降低。