Santoni Giola, Angleman Sara, Welmer Anna-Karin, Mangialasche Francesca, Marengoni Alessandra, Fratiglioni Laura
Aging Research Center, Department of Neurobiology, Care Sciences and Society, Karolinska Institutet and Stockholm University, Stockholm, Sweden.
Aging Research Center, Department of Neurobiology, Care Sciences and Society, Karolinska Institutet and Stockholm University, Stockholm, Sweden; Stockholm Gerontology Research Center, Department of Neurobiology, Care Sciences and Society, Karolinska Institutet, Stockholm, Sweden.
PLoS One. 2015 Mar 3;10(3):e0120077. doi: 10.1371/journal.pone.0120077. eCollection 2015.
Disability, functionality, and morbidity are often used to describe the health of the elderly. Although particularly important when planning health and social services, knowledge about their distribution and aggregation at different ages is limited. We aim to characterize the variation of health status in a 60+ old population using five indicators of health separately and in combination.
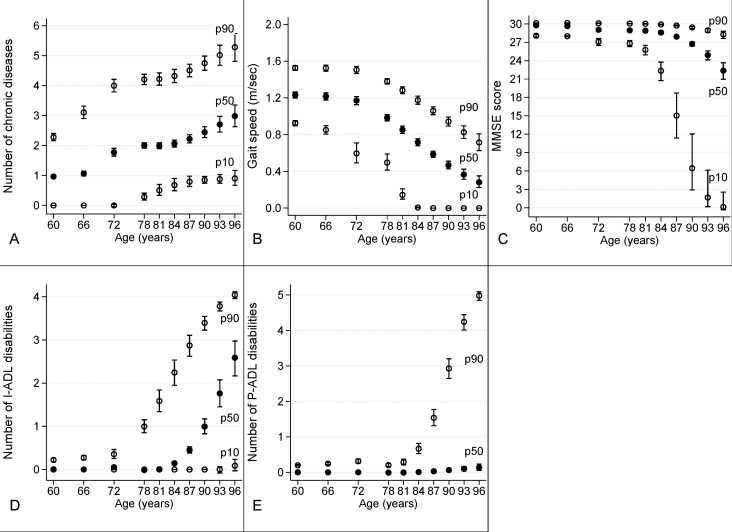
3080 adults 60+ living in Sweden between 2001 and 2004 and participating at the SNAC-K population-based cohort study. Health indicators: number of chronic diseases, gait speed, Mini Mental State Examination (MMSE), disability in instrumental-activities of daily living (I-ADL), and in personal-ADL (P-ADL).
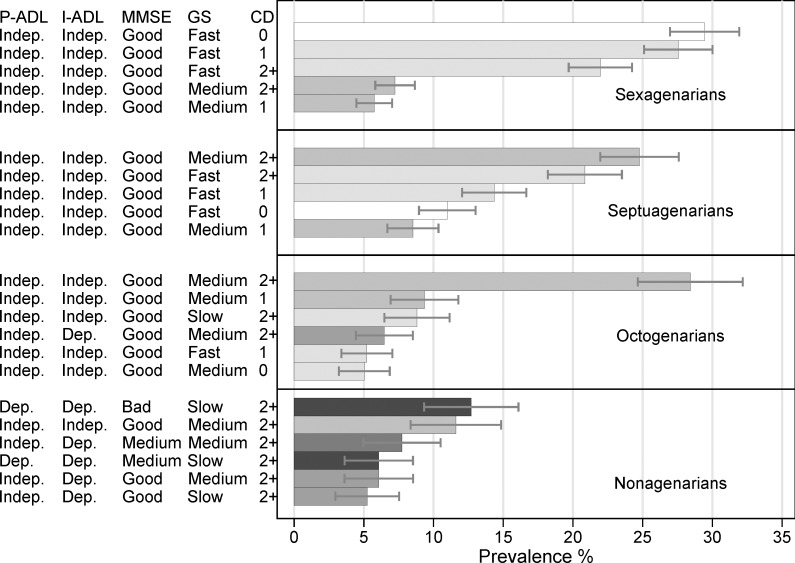
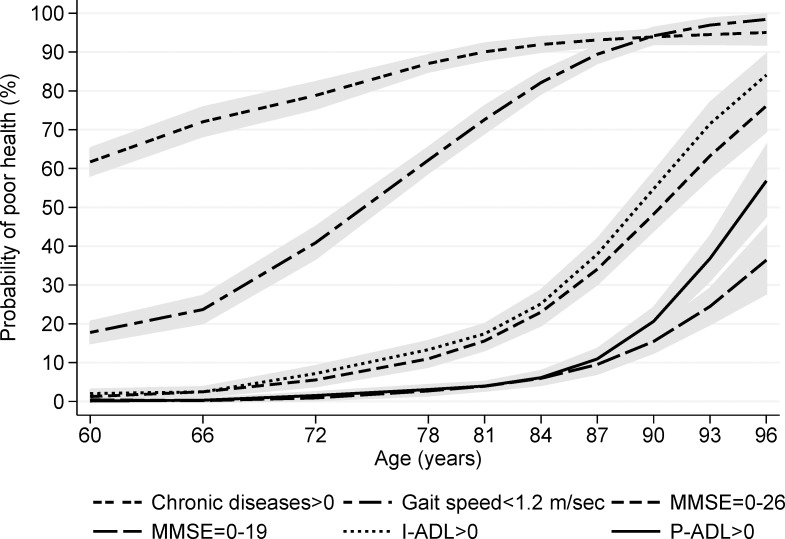
Probability of multimorbidity and probability of slow gait speed were already above 60% and 20% among sexagenarians. Median MMSE and median I-ADL showed good performance range until age 84; median P-ADL was close to zero up to age 90. Thirty% of sexagenarians and 11% of septuagenarians had no morbidity and no impairment, 92% and 80% of them had no disability. Twenty-eight% of octogenarians had multimorbidity but only 27% had some I-ADL disability. Among nonagenarians, 13% had severe disability and impaired functioning while 12% had multimorbidity and slow gait speed.
Age 80-85 is a transitional period when major health changes take place. Until age 80, most people do not have functional impairment or disability, despite the presence of chronic disorders. Disability becomes common only after age 90. This implies an increasing need of medical care after age 70, whereas social care, including institutionalization, becomes a necessity only in nonagenarians.
残疾、功能状态和发病率常被用于描述老年人的健康状况。尽管在规划健康和社会服务时尤为重要,但关于它们在不同年龄段的分布和聚集情况的了解却很有限。我们旨在使用五个健康指标单独及综合地描述60岁及以上人群健康状况的变化。
2001年至2004年期间居住在瑞典且参与了基于人群的SNAC-K队列研究的3080名60岁及以上成年人。健康指标:慢性病数量、步速、简易精神状态检查表(MMSE)、日常生活工具性活动(I-ADL)残疾情况及日常生活个人活动(P-ADL)残疾情况。
在六七十岁人群中,多种疾病并存的概率和步速缓慢的概率已分别超过60%和20%。MMSE中位数和I-ADL中位数在84岁之前表现出良好的性能范围;P-ADL中位数在90岁之前接近零。30%的六七十岁人群无疾病且无功能损害,其中92%和80%无残疾。28%的八九十岁人群患有多种疾病,但只有27%存在一些I-ADL残疾。在九十岁人群中,13%有严重残疾且功能受损,而12%患有多种疾病且步速缓慢。
80 - 85岁是发生重大健康变化的过渡时期。到80岁时,大多数人尽管患有慢性疾病,但没有功能损害或残疾。残疾仅在90岁之后才变得常见。这意味着70岁之后对医疗护理的需求增加,而社会护理,包括机构化护理,仅在九十岁人群中才成为必要。