Aging Research Center, Department of Neurobiology, Care Sciences and Society, Karolinska Institutet and Stockholm University, Stockholm, Sweden.
Department of Geriatrics, Catholic University of Rome, Rome, Italy.
PLoS Med. 2018 Mar 6;15(3):e1002503. doi: 10.1371/journal.pmed.1002503. eCollection 2018 Mar.
Functional decline is a strong health determinant in older adults, and chronic diseases play a major role in this age-related phenomenon. In this study, we explored possible clinical pathways underlying functional heterogeneity in older adults by quantifying the impact of cardiovascular (CV) and neuropsychiatric (NP) chronic diseases and their co-occurrence on trajectories of functional decline.
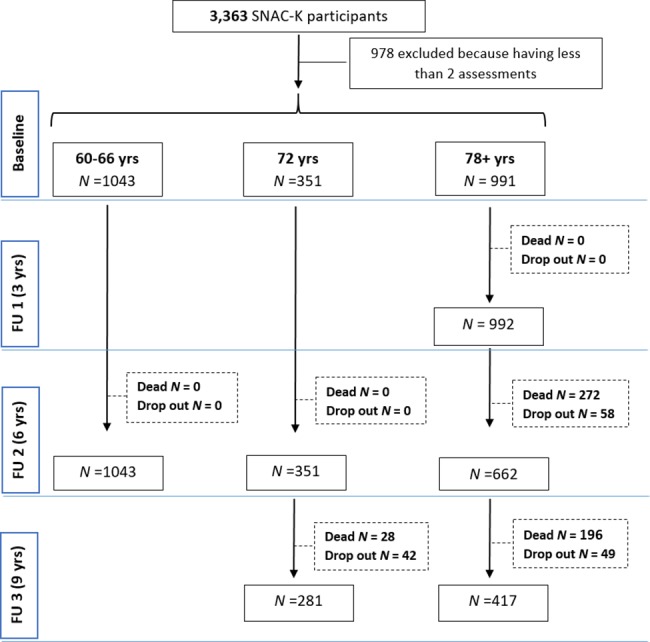
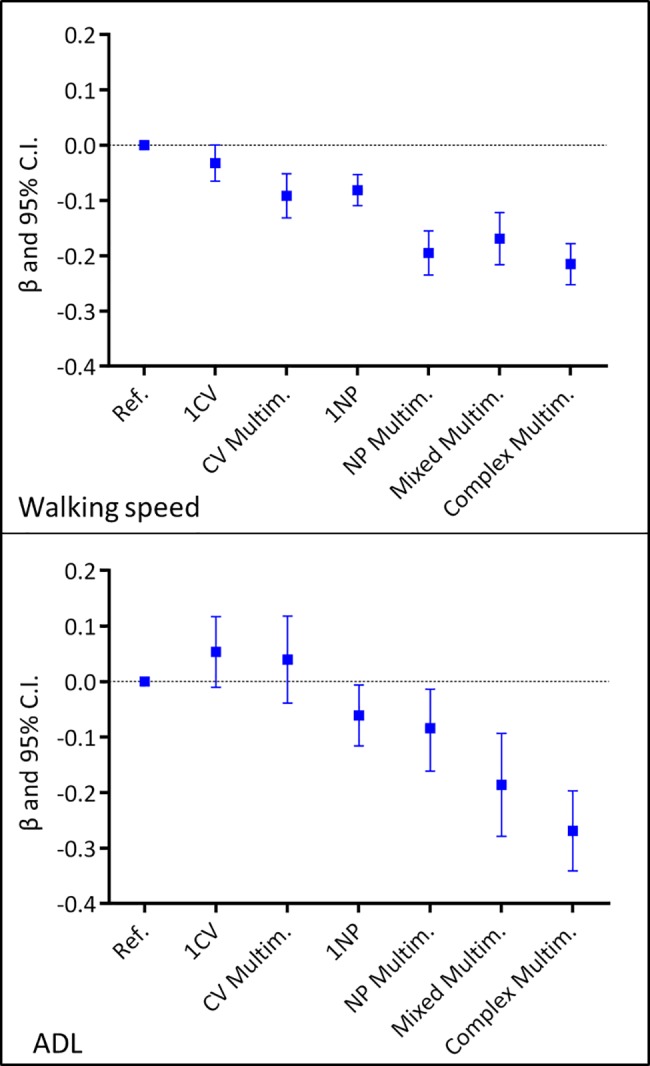
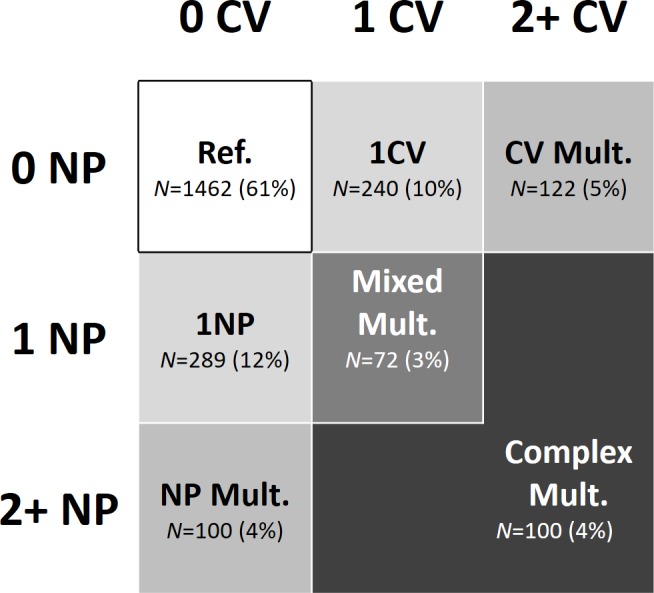
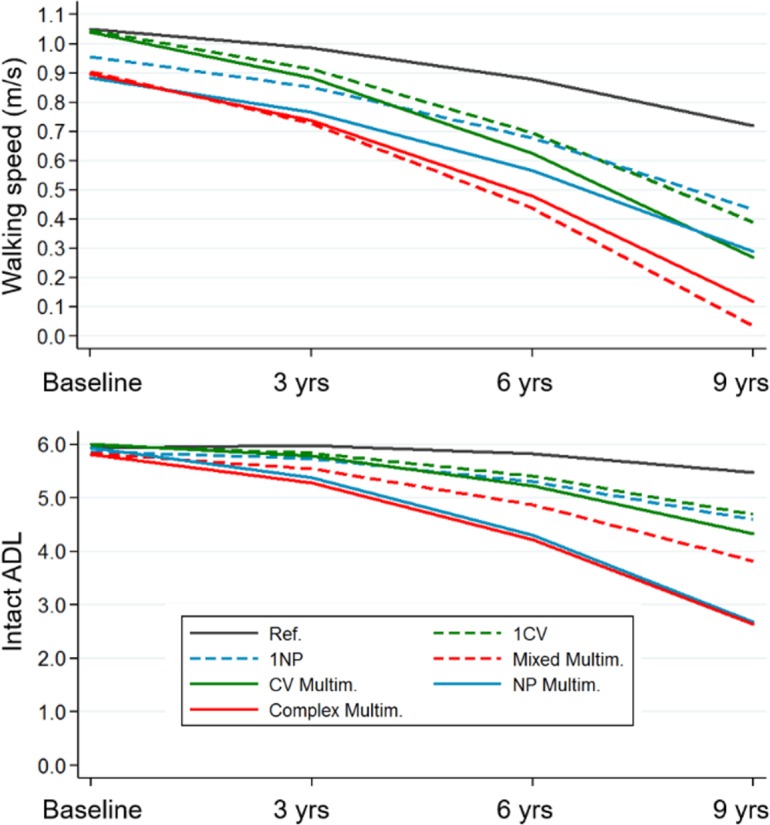
We studied 2,385 people ≥60 years (range 60-101 years) participating in the Swedish National study of Aging and Care in Kungsholmen (SNAC-K). Participants underwent clinical examination at baseline (2001-2004) and every 3 or 6 years for up to 9 years. We grouped participants on the basis of 7 mutually exclusive clinical patterns of 0, 1, or more CV and NP diseases and their co-occurrence, from a group without any CV and NP disease to a group characterised by the presence of CV or NP multimorbidity, accompanied by at least 1 other CV or NP disorder. The group with no CV and/or NP diseases served as the reference group. Functional decline was estimated over 9 years of follow-up by measuring mobility (walking speed, m/s) and independence (ability to carry out six activities of daily living [ADL]). Mixed-effect linear regression models were used (1) to explore the individual-level prognostic predictivity of the different CV and NP clinical patterns at baseline and (2) to quantify the association between the clinical patterns and functional decline at the group level by entering the clinical patterns as time-varying measures. During the 9-year follow-up, participants with multiple CV and NP diseases had the steepest decline in walking speed (up to 0.7 m/s; p < 0.001) and ADL independence (up to three impairments in ADL, p < 0.001) (reference group: participants without any CV and NP disease). When the clinical patterns were analyzed as time varying, isolated CV multimorbidity impacted only walking speed (β -0.1; p < 0.001). Conversely, all the clinical patterns that included at least 1 NP disease were significantly associated with decline in both walking speed (β -0.21--0.08; p < 0.001) and ADL independence (β -0.27--0.06; p < 0.05). Groups with the most complex clinical patterns had 5%-20% lower functioning at follow-up than the reference group. Key limitations of the study include that we did not take into account the specific weight of single diseases and their severity and that the exclusion of participants with less than 2 assessments may have led to an underestimation of the tested associations.
In older adults, different patterns of CV and NP morbidity lead to different trajectories of functional decline over time, a finding that explains part of the heterogeneity observed in older adults' functionality. NP diseases, alone or in association, are prevalent and major determinants of functional decline, whereas isolated CV multimorbidity is associated only with declines in mobility.
功能下降是老年人健康的重要决定因素,而慢性疾病在这一与年龄相关的现象中起着主要作用。在这项研究中,我们通过量化心血管(CV)和神经精神(NP)慢性疾病及其共同发生对功能下降轨迹的影响,探索了老年人功能异质性的可能临床途径。
我们研究了 2385 名年龄在 60 岁及以上(年龄 60-101 岁)的参加瑞典 Kungsholmen 老龄化和护理国家研究(SNAC-K)的人。参与者在基线(2001-2004 年)和每 3 或 6 年进行一次临床检查,最多持续 9 年。我们根据 0、1 或更多 CV 和 NP 疾病及其共同发生的 7 种相互排斥的临床模式,将参与者分组,从没有任何 CV 和 NP 疾病的组到以 CV 或 NP 多种疾病为特征的组,伴有至少 1 种其他 CV 或 NP 疾病。没有 CV 和/或 NP 疾病的组作为参考组。通过测量移动性(行走速度,m/s)和独立性(进行六项日常生活活动的能力),在 9 年的随访中估计功能下降。使用混合效应线性回归模型(1)在基线时探索不同 CV 和 NP 临床模式的个体水平预后预测能力,以及(2)通过将临床模式作为时变措施输入来量化临床模式与功能下降之间的关联。在 9 年的随访中,患有多种 CV 和 NP 疾病的患者在行走速度(最大 0.7 m/s;p < 0.001)和 ADL 独立性(最大 3 项 ADL 受损,p < 0.001)方面下降最快(参考组:无任何 CV 和 NP 疾病的患者)。当将临床模式作为时变因素进行分析时,孤立的 CV 多种疾病仅影响行走速度(β-0.1;p < 0.001)。相反,包括至少 1 种 NP 疾病的所有临床模式都与行走速度(β-0.21-0.08;p < 0.001)和 ADL 独立性(β-0.27-0.06;p < 0.05)的下降显著相关。具有最复杂临床模式的组在随访时的功能比参考组低 5%-20%。该研究的主要局限性包括我们没有考虑单个疾病的具体权重及其严重程度,并且排除少于 2 次评估的参与者可能导致测试关联的低估。
在老年人中,不同的 CV 和 NP 发病模式导致功能随时间的不同轨迹下降,这一发现解释了老年人功能异质性的部分原因。NP 疾病,单独或联合,是功能下降的普遍和主要决定因素,而孤立的 CV 多种疾病仅与移动能力下降有关。