Greenberg David C, Lophatananon Artitaya, Wright Karen A, Muir Kenneth R, Gnanapragasam Vincent J
Public Health England, National Cancer Registration Service [Eastern Office], Cambridge, United Kingdom.
Division of Health Sciences, Warwick Medical School, University of Warwick, Warwick, United Kingdom; Institute of Population Health, University of Manchester, Manchester, United Kingdom.
PLoS One. 2015 Mar 5;10(3):e0119494. doi: 10.1371/journal.pone.0119494. eCollection 2015.
Increasing proportions of men diagnosed with prostate cancer in the UK are presenting with non-metastatic disease. We investigated how treatment trends in this demographic have changed.
Non-metastatic cancers diagnosed from 2000-2010 in the UK Anglian Cancer network stratified by age and risk group were analysed [n = 10,365]. Radiotherapy [RT] and prostatectomy [RP] cancer specific survival [CSS] were further compared [n = 4755].
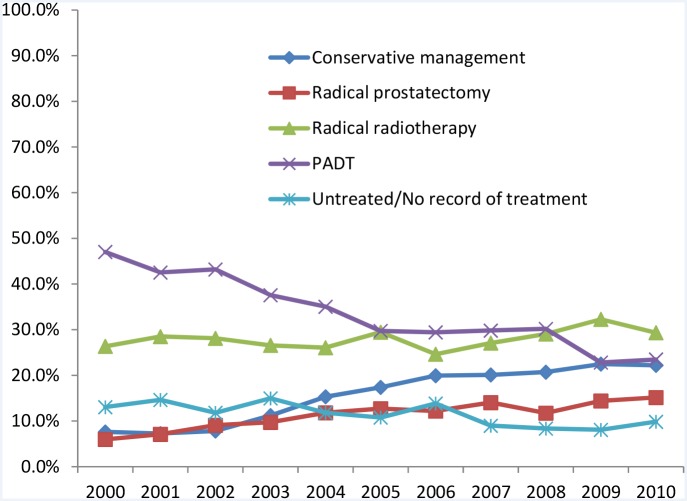
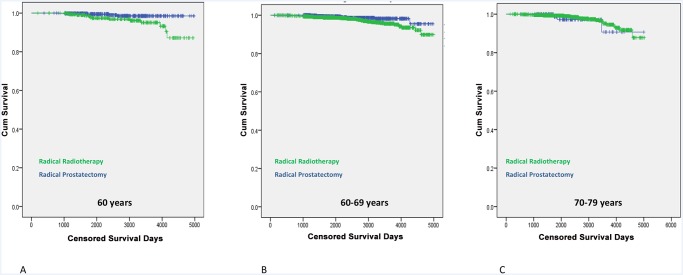
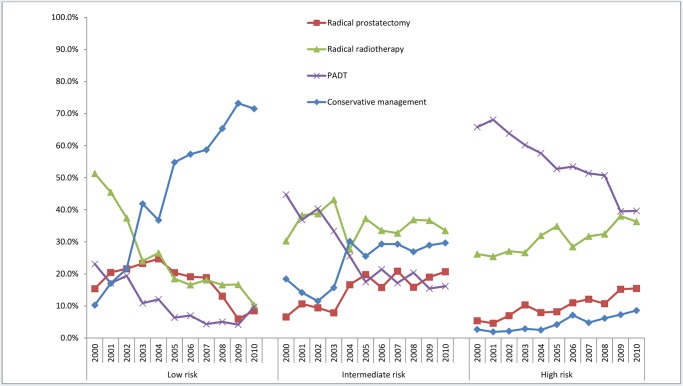
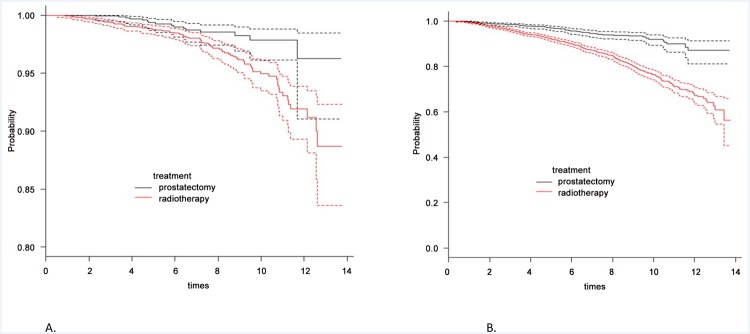
Over the decade we observed a fall in uptake of primary androgen deprivation therapy but a rise in conservative management [CM] and radical therapy [p<0.0001]. CM in particular has become the primary management for low-risk disease by the decade end [p<0.0001]. In high-risk disease however both RP and RT uptake increased significantly but in an age dependent manner [p<0.0001]. Principally, increased RP in younger men and increased RT in men ≥ 70y. In multivariate analysis of radically treated men both high-risk disease [HR 8.0 [2.9-22.2], p<0.0001] and use of RT [HR 1.9 [1.0-3.3], p = 0.024] were significant predictors of a poorer CSM. In age-stratified analysis however, the trend to benefit of RP over RT was seen only in younger men [≤ 60 years] with high-risk disease [p = 0.07]. The numbers needed to treat by RP instead of RT to save one cancer death was 19 for this group but 67 for the overall cohort.
This study has identified significant shifts in non-metastatic prostate cancer management over the last decade. Low-risk disease is now primarily managed by CM while high-risk disease is increasingly treated radically. Treatment of high-risk younger men by RP is supported by evidence of better CSM but this benefit is not evident in older men.
在英国,被诊断为前列腺癌的男性中,非转移性疾病患者的比例日益增加。我们调查了这一人群的治疗趋势是如何变化的。
分析了2000年至2010年在英国盎格鲁癌症网络中按年龄和风险组分层诊断出的非转移性癌症患者[共10365例]。进一步比较了接受放疗[RT]和前列腺切除术[RP]的癌症特异性生存率[CSS][共4755例]。
在这十年间,我们观察到一线雄激素剥夺治疗的采用率下降,但保守治疗[CM]和根治性治疗的采用率上升[P<0.0001]。特别是到这十年结束时,CM已成为低风险疾病的主要治疗方法[P<0.0001]。然而,在高风险疾病中,RP和RT的采用率均显著增加,但呈年龄依赖性[P<0.0001]。主要表现为年轻男性中RP的采用率增加,而70岁及以上男性中RT的采用率增加。在接受根治性治疗的男性的多变量分析中,高风险疾病[风险比8.0[2.9 - 22.2],P<0.0001]和使用RT[风险比1.9[1.0 - 3.3],P = 0.024]都是CSM较差的显著预测因素。然而,在按年龄分层的分析中,仅在患有高风险疾病的年轻男性[≤60岁]中观察到RP优于RT的获益趋势[P = 0.07]。对于该组患者,用RP而非RT治疗以挽救一例癌症死亡所需的治疗人数为19,但在整个队列中为67。
本研究确定了过去十年中非转移性前列腺癌治疗的显著变化。低风险疾病现在主要采用CM治疗,而高风险疾病越来越多地采用根治性治疗。有证据表明,RP治疗高风险年轻男性的CSM更好,但这种获益在老年男性中并不明显。