Academic Urology Group, Department of Surgery and Oncology, University of Cambridge, Box 279 (S4), Cambridge Biomedical Campus, Cambridge, CB2 0QQ, UK.
Addenbrookes Hospital, Department of Urology, Addenbrooke's Hospital, Cambridge, UK.
BMC Med. 2018 Feb 28;16(1):31. doi: 10.1186/s12916-018-1019-5.
The purpose of this study is to validate a new five-tiered prognostic classification system to better discriminate cancer-specific mortality in men diagnosed with primary non-metastatic prostate cancer.
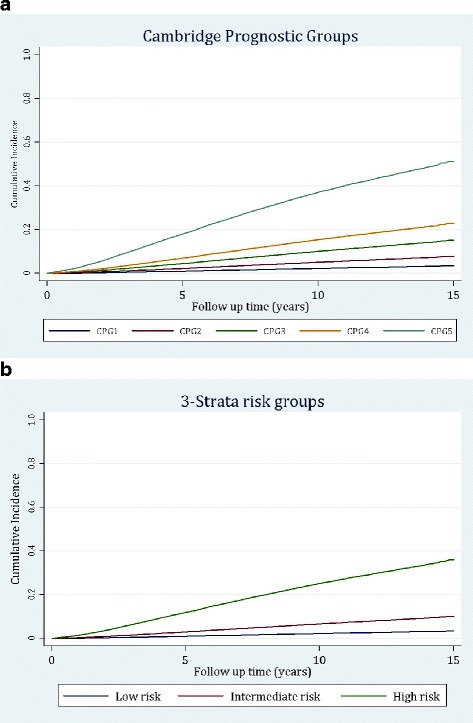
We applied a recently described five-strata model, the Cambridge Prognostic Groups (CPGs 1-5), in two international cohorts and tested prognostic performance against the current standard three-strata classification of low-, intermediate- or high-risk disease. Diagnostic clinico-pathological data for men obtained from the Prostate Cancer data Base Sweden (PCBaSe) and the Singapore Health Study were used. The main outcome measure was prostate cancer mortality (PCM) stratified by age group and treatment modality.
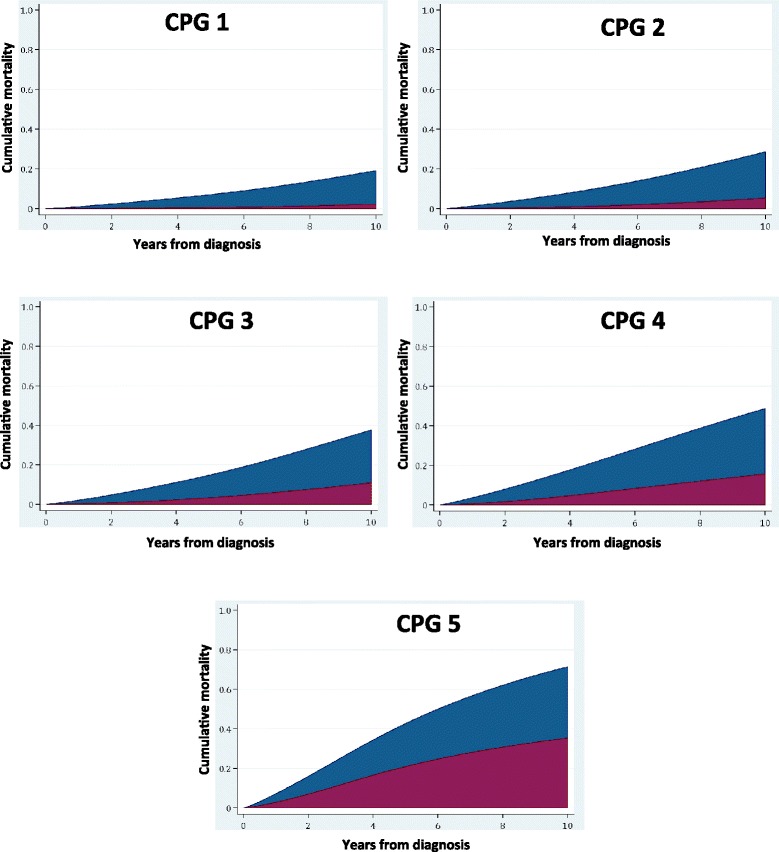
The PCBaSe cohort included 72,337 men, of whom 7162 died of prostate cancer. The CPG model successfully classified men with different risks of PCM with competing risk regression confirming significant intergroup distinction (p < 0.0001). The CPGs were significantly better at stratified prediction of PCM compared to the current three-tiered system (concordance index (C-index) 0.81 vs. 0.77, p < 0.0001). This superiority was maintained for every age group division (p < 0.0001). Also in the ethnically different Singapore cohort of 2550 men with 142 prostate cancer deaths, the CPG model outperformed the three strata categories (C-index 0.79 vs. 0.76, p < 0.0001). The model also retained superior prognostic discrimination in the treatment sub-groups: radical prostatectomy (n = 20,586), C-index 0.77 vs. 074; radiotherapy (n = 11,872), C-index 0.73 vs. 0.69; and conservative management (n = 14,950), C-index 0.74 vs. 0.73. The CPG groups that sub-divided the old intermediate-risk (CPG2 vs. CPG3) and high-risk categories (CPG4 vs. CPG5) significantly discriminated PCM outcomes after radical therapy or conservative management (p < 0.0001).
This validation study of nearly 75,000 men confirms that the CPG five-tiered prognostic model has superior discrimination compared to the three-tiered model in predicting prostate cancer death across different age and treatment groups. Crucially, it identifies distinct sub-groups of men within the old intermediate-risk and high-risk criteria who have very different prognostic outcomes. We therefore propose adoption of the CPG model as a simple-to-use but more accurate prognostic stratification tool to help guide management for men with newly diagnosed prostate cancer.
本研究旨在验证一种新的五层级预后分类系统,以更好地区分诊断为原发性非转移性前列腺癌男性的癌症特异性死亡率。
我们应用了最近描述的五层次模型,即剑桥预后组(CPGs 1-5),在两个国际队列中进行了测试,并将预后性能与当前低、中或高危疾病的三层次分类进行了比较。使用了来自前列腺癌数据库瑞典(PCBaSe)和新加坡健康研究的男性临床病理诊断数据。主要观察指标为按年龄组和治疗方式分层的前列腺癌死亡率(PCM)。
PCBaSe 队列包括 72337 名男性,其中 7162 人死于前列腺癌。CPG 模型成功地对具有不同 PCM 风险的男性进行了分类,竞争风险回归证实了组间的显著差异(p<0.0001)。CPGs 在分层预测 PCM 方面明显优于当前的三层次系统(一致性指数(C 指数)0.81 与 0.77,p<0.0001)。这一优势在每个年龄组都得到了保持(p<0.0001)。在 2550 名男性的新加坡队列中,有 142 人死于前列腺癌,CPG 模型也优于三层次类别(C 指数 0.79 与 0.76,p<0.0001)。该模型在治疗亚组中也保持了优越的预后区分能力:根治性前列腺切除术(n=20586),C 指数 0.77 与 0.74;放疗(n=11872),C 指数 0.73 与 0.69;保守治疗(n=14950),C 指数 0.74 与 0.73。旧的中间风险(CPG2 与 CPG3)和高风险(CPG4 与 CPG5)分组的 CPG 组显著区分了根治性治疗或保守治疗后的 PCM 结局(p<0.0001)。
这项对近 75000 名男性的验证研究证实,CPG 五层次预后模型在预测不同年龄和治疗组的前列腺癌死亡方面具有优于三层次模型的区分能力。至关重要的是,它在旧的中间风险和高风险标准内确定了具有非常不同预后结果的男性亚组。因此,我们建议采用 CPG 模型作为一种简单易用但更准确的预后分层工具,以帮助指导新诊断为前列腺癌的男性的治疗管理。