Hwang Jyh-Chang, Jiang Ming-Yan, Lu Yi-Hua, Wang Charn-Ting
Division of Nephrology, Chi Mei Medical Center, Tainan, Taiwan; Department of Hospital and Health Care Administration, Chia Nan University of Pharmacy and Science, Tainan, Taiwan.
Division of Nephrology, Chi Mei Medical Center, Tainan, Taiwan.
PLoS One. 2015 Mar 20;10(3):e0120266. doi: 10.1371/journal.pone.0120266. eCollection 2015.
A high sensitivity C-reactive protein to albumin ratio (hs-CRP/Alb) predicts mortality risk in patients with acute kidney injury. However, it varies dynamically. This study was conducted to evaluate whether a variation of this marker was associated with long-term outcome in clinically stable hemodialysis (HD) patients.
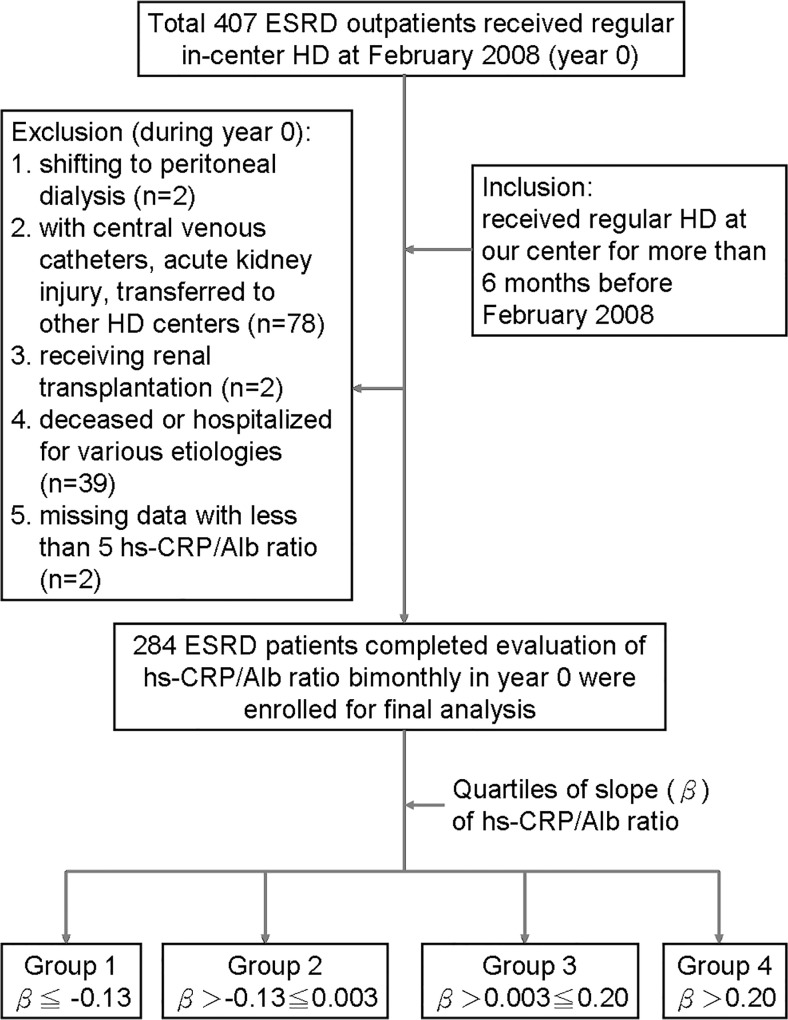
hs-CRP/Alb was checked bimonthly in 284 clinically stable HD outpatients throughout all of 2008. Based on the "slope" of trend equation derived from 5-6 hs-CRP/alb ratios for each patient, the total number of patients was divided into quartiles--Group 1: β≦ -0.13, n = 71; group 2: β>-0.13≦0.003; n = 71, group 3: β>0.003≦0.20; and group 4: β>0.20, n = 71. The observation period was from January 1, 2009 to August 31, 2012.
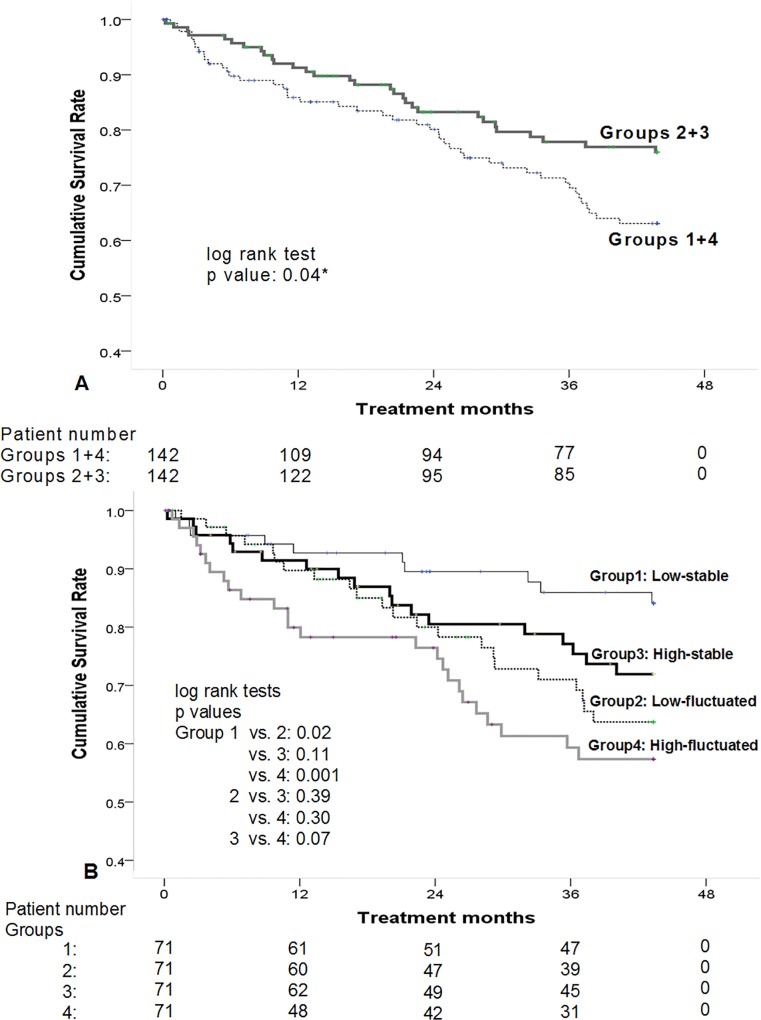
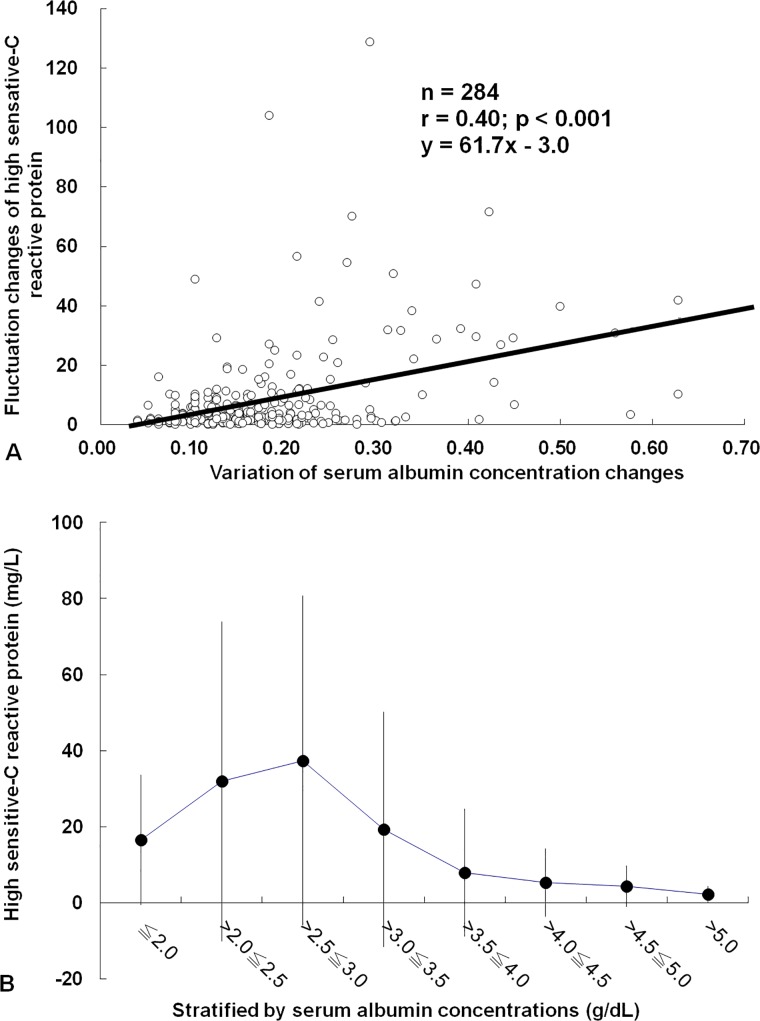
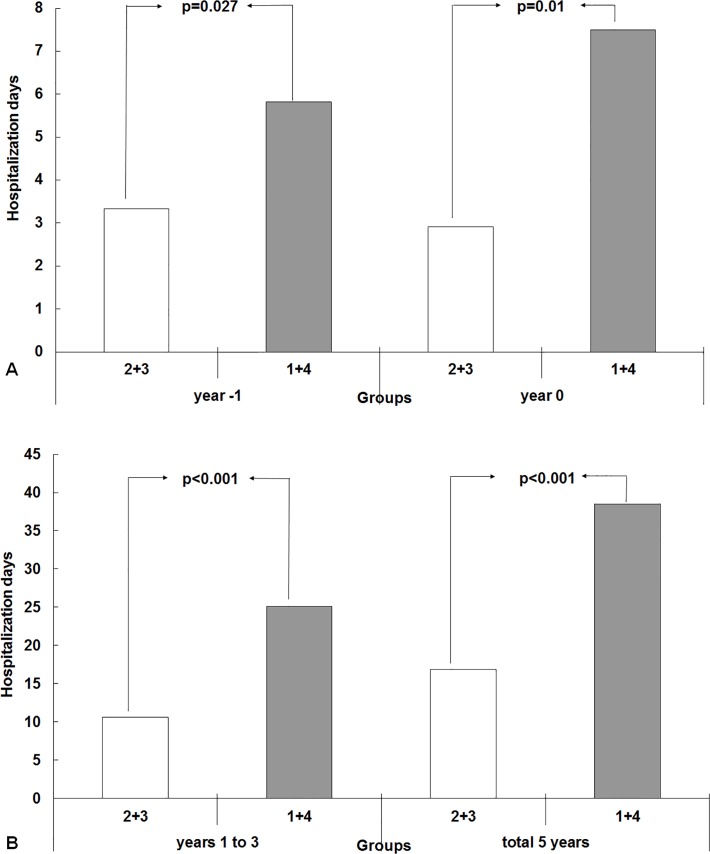
Group 1+4 showed a worse long-term survival (p = 0.04) and a longer 5-year hospitalization stay than Group 2+3 (38.7±44.4 vs. 16.7±22.4 days, p<0.001). Group 1+4 were associated with older age (OR = 1.03, 95% CI = 1.01-1.05) and a high prevalence of congestive heart failure (OR = 2.02, 95% CI = 1.00-4.11). Standard deviation (SD) of hs-CRP/Alb was associated with male sex (β = 0.17, p = 0.003), higher Davies co-morbidity score (β = 0.16, p = 0.03), and baseline hs-CRP (β = 0.39, p<0.001). Patients with lower baseline and stable trend of hs-CRP/Alb had a better prognosis. By multivariate Cox proportional methods, SD of hs-CRP/alb (HR: 1.05, 95% CI: 1.01-1.08) rather than baseline hs-CRP/Alb was an independent predictive factor for long-term mortality after adjusting for sex and HD vintage.
Clinically stable HD patients with a fluctuating variation of hs-CRP/Alb are characterized by old age, and more co-morbidity, and they tend to have longer subsequent hospitalization stay and higher mortality risk.
高敏C反应蛋白与白蛋白比值(hs-CRP/Alb)可预测急性肾损伤患者的死亡风险。然而,该比值会动态变化。本研究旨在评估这一标志物的变化是否与临床稳定的血液透析(HD)患者的长期预后相关。
在2008年全年,对284例临床稳定的HD门诊患者每两个月检测一次hs-CRP/Alb。根据每位患者5 - 6次hs-CRP/Alb比值得出的趋势方程“斜率”,将患者总数分为四个四分位数组——第1组:β≤ -0.13,n = 71;第2组:β> -0.13≤0.003,n = 71;第3组:β> 0.003≤0.20;第4组:β> 0.20,n = 71。观察期为2009年1月1日至2012年8月31日。
第1组 + 第4组显示出较差的长期生存率(p = 0.04),且5年住院时间长于第2组 + 第3组(38.7±44.4天对16.7±22.4天,p<0.001)。第1组 + 第4组与高龄(OR = 1.03,95%CI = 1.01 - 1.05)和充血性心力衰竭的高患病率(OR = 2.02,95%CI = 1.00 - 4.11)相关。hs-CRP/Alb的标准差与男性(β = 0.17,p = 0.003)、较高的戴维斯合并症评分(β = 0.16,p = 0.03)以及基线hs-CRP(β = 0.39,p<0.001)相关。hs-CRP/Alb基线较低且趋势稳定的患者预后较好。通过多变量Cox比例法,调整性别和HD透析龄后,hs-CRP/alb的标准差(HR:1.05,95%CI:1.01 - 1.08)而非基线hs-CRP/Alb是长期死亡率的独立预测因素。
hs-CRP/Alb波动变化的临床稳定HD患者具有年龄较大、合并症较多的特点,且其后住院时间往往更长,死亡风险更高。