Intensive Care Unit, Emergency Medicine Discipline, Hospital das Clínicas, Universidade de São Paulo, São Paulo, Brazil.
PLoS One. 2013;8(3):e59321. doi: 10.1371/journal.pone.0059321. Epub 2013 Mar 12.
Residual inflammation at ICU discharge may have impact upon long-term mortality. However, the significance of ongoing inflammation on mortality after ICU discharge is poorly described. C-reactive protein (CRP) and albumin are measured frequently in the ICU and exhibit opposing patterns during inflammation. Since infection is a potent trigger of inflammation, we hypothesized that CRP levels at discharge would correlate with long-term mortality in septic patients and that the CRP/albumin ratio would be a better marker of prognosis than CRP alone.
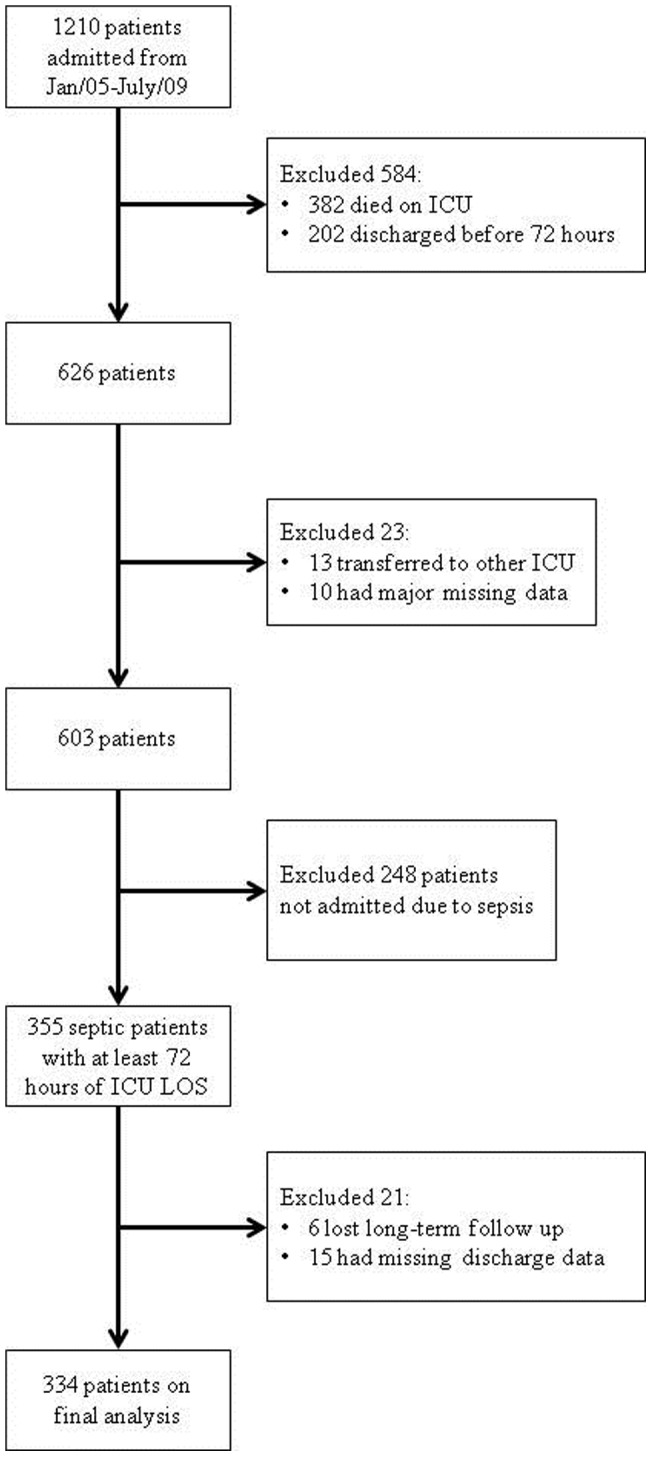
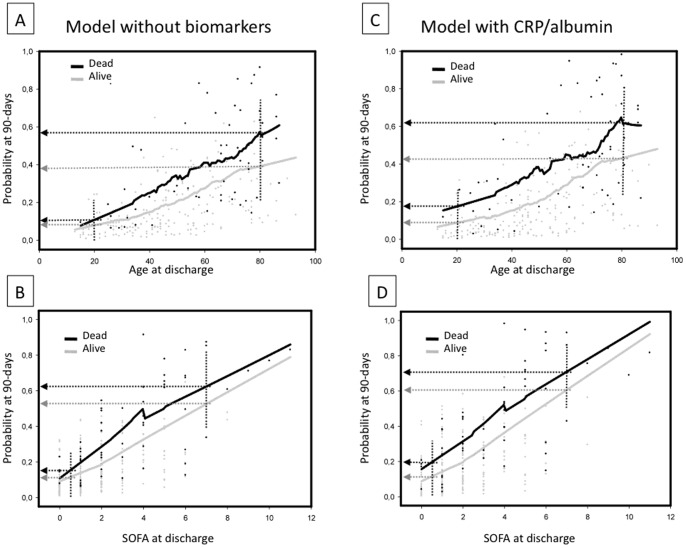
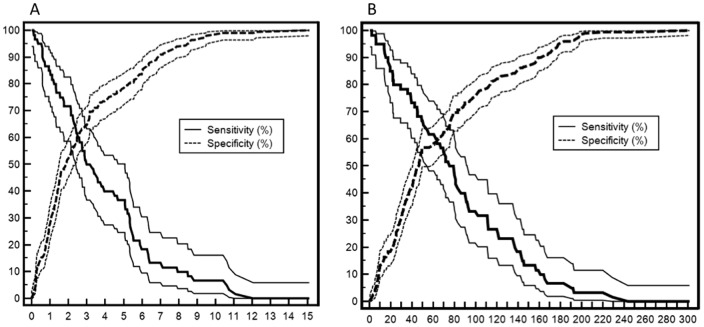
We evaluated 334 patients admitted to the ICU as a result of severe sepsis or septic shock who were discharged alive after a minimum of 72 hours in the ICU. We evaluated the performance of both CRP and CRP/albumin to predict mortality at 90 days after ICU discharge. Two multivariate logistic models were generated based on measurements at discharge: one model included CRP (Model-CRP), and the other included the CRP/albumin ratio (Model-CRP/albumin).
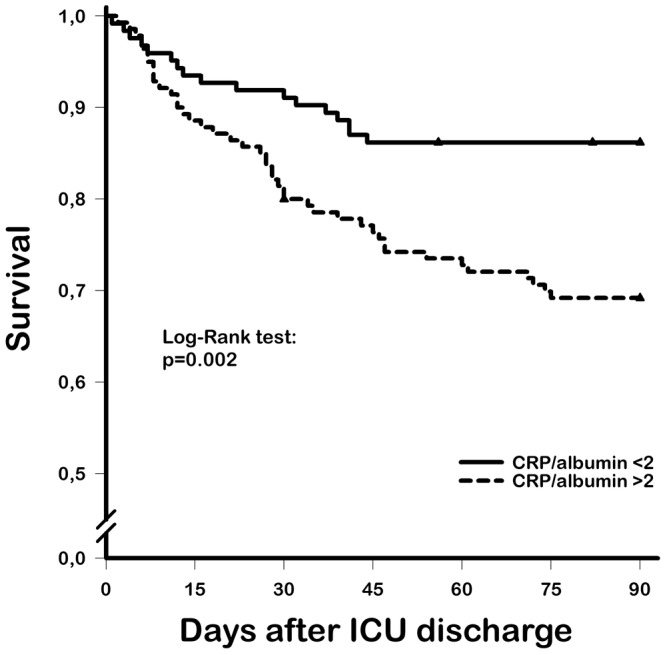
There were 229 (67%) and 111 (33%) patients with severe sepsis and septic shock, respectively. During the 90 days of follow-up, 73 (22%) patients died. CRP/albumin ratios at admission and at discharge were associated with a poor outcome and showed greater accuracy than CRP alone at these time points (p = 0.0455 and p = 0.0438, respectively). CRP levels and the CRP/albumin ratio were independent predictors of mortality at 90 days (Model-CRP: adjusted OR 2.34, 95% CI 1.14-4.83, p = 0.021; Model-CRP/albumin: adjusted OR 2.18, 95% CI 1.10-4.67, p = 0.035). Both models showed similar accuracy (p = 0.2483). However, Model-CRP was not calibrated.
Residual inflammation at ICU discharge assessed using the CRP/albumin ratio is an independent risk factor for mortality at 90 days in septic patients. The use of the CRP/albumin ratio as a long-term marker of prognosis provides more consistent results than standard CRP values alone.
重症监护病房(ICU)出院时的残留炎症可能对长期死亡率有影响。然而,炎症持续存在对 ICU 出院后死亡率的意义描述不足。C 反应蛋白(CRP)和白蛋白在 ICU 中经常测量,在炎症期间表现出相反的模式。由于感染是炎症的有力触发因素,我们假设出院时的 CRP 水平与脓毒症患者的长期死亡率相关,并且 CRP/白蛋白比值将比单独 CRP 更好地预测预后。
我们评估了 334 名因严重败血症或败血症性休克而入住 ICU 的患者,这些患者在 ICU 中至少存活 72 小时后出院。我们评估了 CRP 和 CRP/白蛋白在预测 ICU 出院后 90 天死亡率方面的表现。根据出院时的测量值生成了两个多变量逻辑模型:一个模型包括 CRP(CRP 模型),另一个模型包括 CRP/白蛋白比值(CRP/白蛋白模型)。
分别有 229 名(67%)和 111 名(33%)患者患有严重败血症和败血症性休克。在 90 天的随访期间,73 名(22%)患者死亡。入院和出院时的 CRP/白蛋白比值与不良预后相关,并且在这些时间点的准确性高于单独 CRP(p = 0.0455 和 p = 0.0438)。CRP 水平和 CRP/白蛋白比值是 90 天死亡率的独立预测因素(CRP 模型:调整后的 OR 2.34,95%CI 1.14-4.83,p = 0.021;CRP/白蛋白模型:调整后的 OR 2.18,95%CI 1.10-4.67,p = 0.035)。两个模型的准确性相似(p = 0.2483)。然而,CRP 模型未进行校准。
使用 CRP/白蛋白比值评估 ICU 出院时的残留炎症是脓毒症患者 90 天死亡率的独立危险因素。使用 CRP/白蛋白比值作为长期预后标志物比单独使用标准 CRP 值提供更一致的结果。