Rapaport M H, Nierenberg A A, Schettler P J, Kinkead B, Cardoos A, Walker R, Mischoulon D
Department of Psychiatry and Behavioral Sciences, Emory University School of Medicine, Atlanta, GA, USA.
Depression Clinical and Research Program, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA.
Mol Psychiatry. 2016 Jan;21(1):71-9. doi: 10.1038/mp.2015.22. Epub 2015 Mar 24.
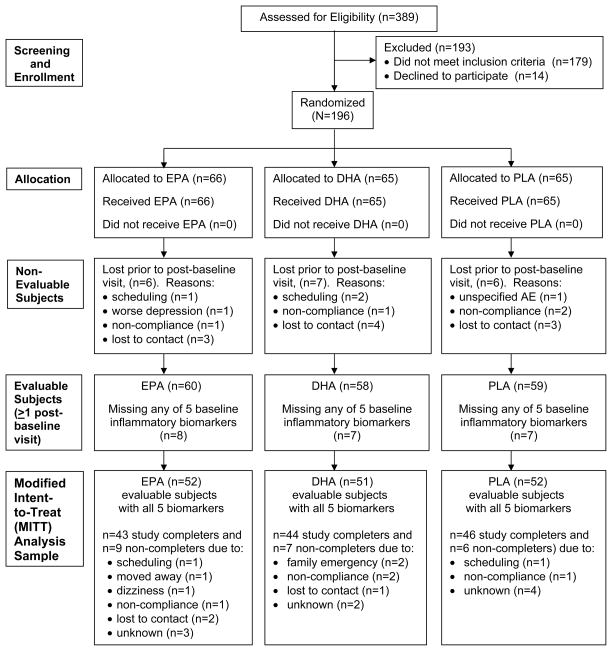
This study explores whether inflammatory biomarkers act as moderators of clinical response to omega-3 (n-3) fatty acids in subjects with major depressive disorder (MDD). One hundred fifty-five subjects with Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV) MDD, a baseline 17-item Hamilton Depression Rating Scale (HAM-D-17) score ⩾ 15 and baseline biomarker data (interleukin (IL)-1ra, IL-6, high-sensitivity C-reactive protein (hs-CRP), leptin and adiponectin) were randomized between 18 May 2006 and 30 June 2011 to 8 weeks of double-blind treatment with eicosapentaenoic acid (EPA)-enriched n-3 1060 mg day(-1), docosahexaenoic acid (DHA)-enriched n-3 900 mg day(-1) or placebo. Outcomes were determined using mixed model repeated measures analysis for 'high' and 'low' inflammation groups based on individual and combined biomarkers. Results are presented in terms of standardized treatment effect size (ES) for change in HAM-D-17 from baseline to treatment week 8. Although overall treatment group differences were negligible (ES=-0.13 to +0.04), subjects with any 'high' inflammation improved more on EPA than placebo (ES=-0.39) or DHA (ES=-0.60) and less on DHA than placebo (ES=+0.21); furthermore, EPA-placebo separation increased with increasing numbers of markers of high inflammation. Subjects randomized to EPA with 'high' IL-1ra or hs-CRP or low adiponectin ('high' inflammation) had medium ES decreases in HAM-D-17 scores vs subjects 'low' on these biomarkers. Subjects with 'high' hs-CRP, IL-6 or leptin were less placebo-responsive than subjects with low levels of these biomarkers (medium to large ES differences). Employing multiple markers of inflammation facilitated identification of a more homogeneous cohort of subjects with MDD responding to EPA vs placebo in our cohort. Studies are needed to replicate and extend this proof-of-concept work.
本研究探讨炎症生物标志物是否作为重度抑郁症(MDD)患者对ω-3(n-3)脂肪酸临床反应的调节因素。155名符合《精神疾病诊断与统计手册》第4版(DSM-IV)中MDD诊断标准、汉密尔顿抑郁量表17项(HAM-D-17)基线评分≥15且有基线生物标志物数据(白细胞介素(IL)-1ra、IL-6、高敏C反应蛋白(hs-CRP)、瘦素和脂联素)的受试者于2006年5月18日至2011年6月30日期间被随机分为三组,分别接受为期8周的双盲治疗,治疗方案为:富含二十碳五烯酸(EPA)的n-3 1060毫克/天、富含二十二碳六烯酸(DHA)的n-3 900毫克/天或安慰剂。基于个体和组合生物标志物,使用混合模型重复测量分析来确定“高”炎症组和“低”炎症组的结果。结果以从基线到治疗第8周HAM-D-17变化的标准化治疗效应大小(ES)表示。尽管总体治疗组差异可忽略不计(ES=-0.13至+0.04),但任何“高”炎症受试者接受EPA治疗后的改善程度均高于安慰剂(ES=-0.39)或DHA(ES=-0.60),接受DHA治疗后的改善程度低于安慰剂(ES=+0.21);此外,EPA与安慰剂之间的差异随着高炎症标志物数量的增加而增大。随机接受EPA治疗且IL-1ra或hs-CRP“高”或脂联素“低”(“高”炎症)的受试者,其HAM-D-17评分的ES下降幅度中等,而这些生物标志物“低”的受试者则不然。hs-CRP、IL-6或瘦素“高”的受试者比这些生物标志物水平低的受试者对安慰剂的反应性更低(ES差异为中等至大)。在我们的队列中,使用多种炎症标志物有助于识别出一组对EPA与安慰剂反应更一致的MDD受试者。需要开展研究来重复和扩展这项概念验证工作。