Bachaspatimayum Romita, Haokip Thangjamang, Zamzachin G, Devi Yanglem Elizabeth
Department of Dermatology, Venereology and Leprology, Regional Institute of Medical Science, Imphal, Manipur, India.
Indian J Dermatol. 2015 Mar-Apr;60(2):215. doi: 10.4103/0019-5154.152607.
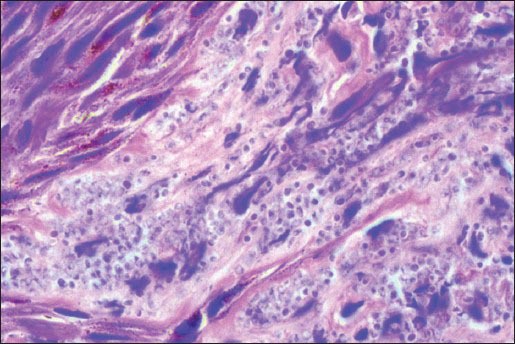
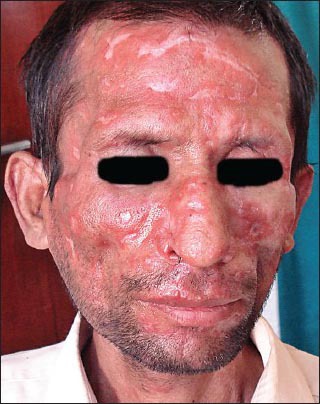
A 40-year-old male human immunodeficiency virus (HIV) -positive patient on highly active antiretroviral therapy (HAART) developed bilateral cervical lymphadenopathy with fine needle aspiration cytology (FNAC) showing yeast cells of Penicillium marneffei. The adenopathy disappeared after 9 months of itraconazole therapy at a dose of 200 mg/day. Seven years later and 2 days following second-line HAART, the patient presented with generalized papulonodules and ulceronecrotic lesions. Biopsy of the skin lesion revealed plenty of yeast forms dividing by binary fission morphologically resembling Penicillium marneffei. Significant improvement was observed at 2 weeks of starting itraconazole 400 mg/day. After 3 months, the dose was reduced to 200 mg/day and advised to continue for 6 months. Penicillosis presenting initially in the form of cervical adenopathy and later, developing typical skin lesions rapidly progressing to ulcerative and necrotic erosions may be due to continued immunosuppression followed by immune reconstitution inflammatory syndrome (IRIS).
一名40岁的男性人类免疫缺陷病毒(HIV)阳性患者,正在接受高效抗逆转录病毒治疗(HAART),出现双侧颈部淋巴结病,细针穿刺细胞学检查(FNAC)显示马尔尼菲青霉菌酵母细胞。接受每日200毫克伊曲康唑治疗9个月后,淋巴结病消失。7年后,在二线HAART治疗2天后,患者出现全身性丘疹结节和溃疡坏死性病变。皮肤病变活检显示大量酵母形态,通过二分裂繁殖,形态上类似于马尔尼菲青霉菌。开始每日400毫克伊曲康唑治疗2周后观察到明显改善。3个月后,剂量减至每日200毫克,并建议持续6个月。最初表现为颈部淋巴结病,随后迅速发展为典型皮肤病变并进展为溃疡性和坏死性糜烂的青霉病,可能是由于持续免疫抑制后发生免疫重建炎症综合征(IRIS)。