Neirynck Nathalie, Glorieux Griet, Schepers Eva, Verbeke Francis, Vanholder Raymond
Nephrology Section, Department of Internal Medicine, Ghent University Hospital, Ghent, Belgium.
PLoS One. 2015 Mar 30;10(3):e0122073. doi: 10.1371/journal.pone.0122073. eCollection 2015.
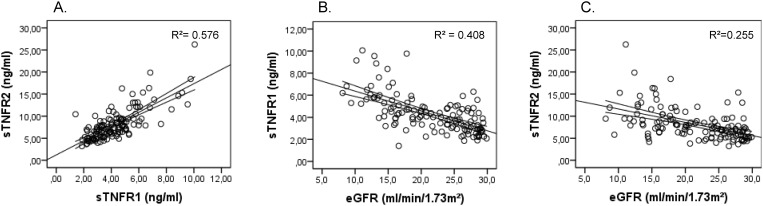
Soluble tumor necrosis factor receptors 1 (sTNFR1) and 2 (sTNFR2) have been associated to progression of renal failure, end stage renal disease and mortality in early stages of chronic kidney disease (CKD), mostly in the context of diabetic nephropathy. The predictive value of these markers in advanced stages of CKD irrespective of the specific causes of kidney disease has not yet been defined. In this study, the relationship between sTNFR1 and sTNFR2 and the risk for adverse cardiovascular events (CVE) and all-cause mortality was investigated in a population with CKD stage 4-5, not yet on dialysis, to minimize the confounding by renal function.
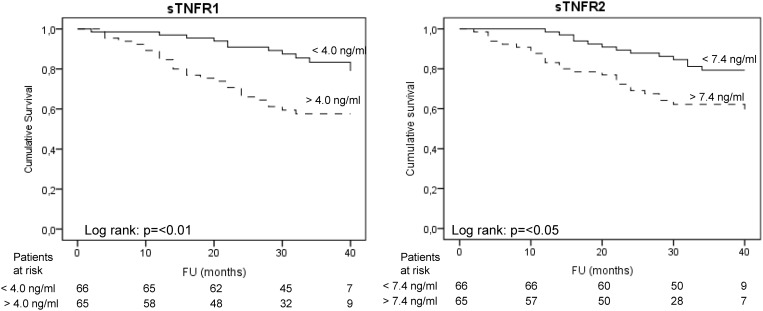
In 131 patients, CKD stage 4-5, sTNFR1, sTNFR2 were analysed for their association to a composite endpoint of all-cause mortality or first non-fatal CVE by univariate and multivariate Cox proportional hazards models. In the multivariate models, age, gender, CRP, eGFR and significant comorbidities were included as covariates.
During a median follow-up of 33 months, 40 events (30.5%) occurred of which 29 deaths (22.1%) and 11 (8.4%) first non-fatal CVE. In univariate analysis, the hazard ratios (HR) of sTNFR1 and sTNFR2 for negative outcome were 1.49 (95% confidence interval (CI): 1.28-1.75) and 1.13 (95% CI: 1.06-1.20) respectively. After adjustment for clinical covariables (age, CRP, diabetes and a history of cardiovascular disease) both sTNFRs remained independently associated to outcomes (HR: sTNFR1: 1.51, 95% CI: 1.30-1.77; sTNFR2: 1.13, 95% CI: 1.06-1.20). A subanalysis of the non-diabetic patients in the study population confirmed these findings, especially for sTNFR1.
sTNFR1 and sTNFR2 are independently associated to all-cause mortality or an increased risk for cardiovascular events in advanced CKD irrespective of the cause of kidney disease.
可溶性肿瘤坏死因子受体1(sTNFR1)和2(sTNFR2)与肾衰竭进展、终末期肾病以及慢性肾脏病(CKD)早期的死亡率相关,这主要发生在糖尿病肾病的背景下。这些标志物在CKD晚期的预测价值尚未明确,而不考虑肾脏疾病的具体病因。在本研究中,我们在尚未接受透析的4-5期CKD患者中,研究了sTNFR1和sTNFR2与不良心血管事件(CVE)风险及全因死亡率之间的关系,以尽量减少肾功能的混杂影响。
对131例4-5期CKD患者的sTNFR1和sTNFR2进行分析,通过单因素和多因素Cox比例风险模型研究其与全因死亡率或首次非致命性CVE复合终点的相关性。在多因素模型中,纳入年龄、性别、CRP、估算肾小球滤过率(eGFR)和显著的合并症作为协变量。
在中位随访33个月期间,发生了40起事件(30.5%),其中29例死亡(22.1%),11例(8.4%)首次非致命性CVE。单因素分析中,sTNFR1和sTNFR2出现不良结局的风险比(HR)分别为1.49(95%置信区间(CI):1.28-1.75)和1.13(95%CI:1.06-1.20)。在对临床协变量(年龄、CRP、糖尿病和心血管疾病史)进行调整后,两种sTNFR仍与结局独立相关(HR:sTNFR1:1.51,95%CI:1.30-1.77;sTNFR2:1.13,95%CI:1.06-1.20)。对研究人群中非糖尿病患者的亚组分析证实了这些发现,尤其是对于sTNFR1。
无论肾脏疾病病因如何,sTNFR1和sTNFR2均与晚期CKD的全因死亡率或心血管事件风险增加独立相关。