Cabrero Monica, Jabbour Elias, Ravandi Farhad, Bohannan Zach, Pierce Sherry, Kantarjian Hagop M, Garcia-Manero Guillermo
Department of Leukemia, The University of Texas MD Anderson Cancer Center, Houston, TX, United States.
Department of Leukemia, The University of Texas MD Anderson Cancer Center, Houston, TX, United States.
Leuk Res. 2015 May;39(5):520-4. doi: 10.1016/j.leukres.2015.03.006. Epub 2015 Mar 20.
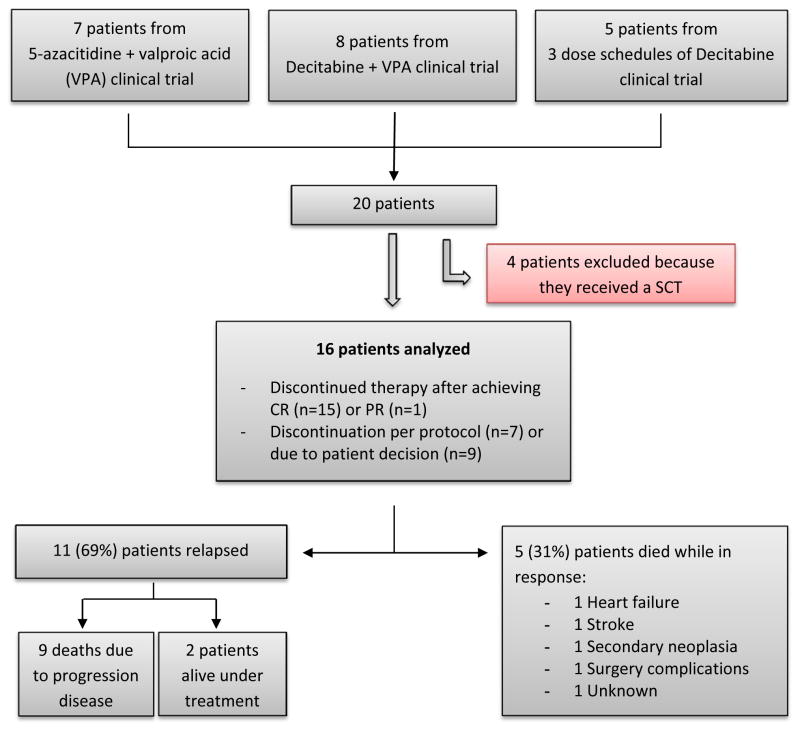
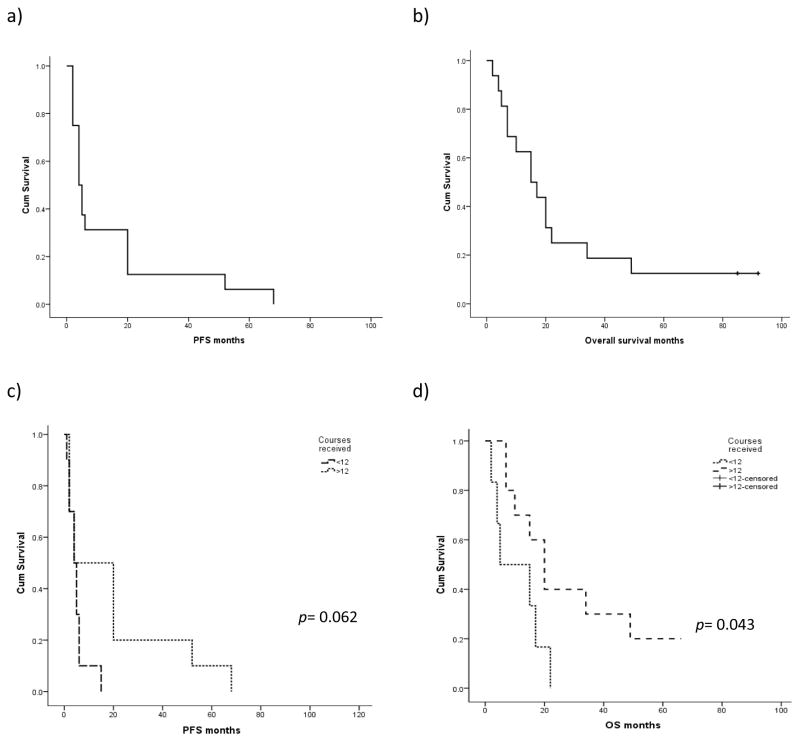
Hypomethylating agents (HMA), such as 5-azacitidine or decitabine, are currently used to treat patients with myelodysplastic syndromes (MDS) or acute myeloid leukemia (AML) until treatment failure. However, the outcomes for patients who discontinue therapy after achieving partial response (PR) or complete remission (CR) but before treatment failure have not been reported. We present a series of 16 patients with higher-risk MDS (n=5; 31%) or AML (n=11; 69%) who achieved PR (n=1) or CR (n=15) and stopped HMA therapy while in response in the context of clinical trials. They received a median of 12 courses (range 1-24) and achieved response after a median of 1 course of therapy (1-4). Loss of response after discontinuation of therapy was rapid, with a median progression-free survival of 4 months (95% CI: 2-6). Median overall survival (OS) from the time of therapy discontinuation was 15 months (95% CI: 6-24). Patients who received 12 cycles of therapy or more had significantly better OS (median: 20 months [95% CI: 12-27]) than those who received fewer than 12 cycles (median: 4 months [95% CI: 1-8]) (p=0.043). Poor-risk cytogenetics were also associated with lower 1-year OS (33% versus 69%; p=0.046). According to these results and considering the poor prognosis after HMA failure, HMA interruption should be avoided once a sustained response has been achieved.
低甲基化药物(HMA),如5-氮杂胞苷或地西他滨,目前用于治疗骨髓增生异常综合征(MDS)或急性髓系白血病(AML)患者,直至治疗失败。然而,对于在达到部分缓解(PR)或完全缓解(CR)后但在治疗失败前停止治疗的患者的预后情况尚未见报道。我们报告了16例高危MDS患者(n = 5;31%)或AML患者(n = 11;69%),他们在临床试验中达到PR(n = 1)或CR(n = 15)并在缓解期停止HMA治疗。他们接受的疗程中位数为12个疗程(范围1 - 24个疗程),治疗1个疗程(1 - 4个疗程)后达到缓解。治疗中断后缓解消失迅速,无进展生存期中位数为4个月(95%置信区间:2 - 6个月)。从治疗中断时起的总生存期(OS)中位数为15个月(95%置信区间:6 - 24个月)。接受12个或更多疗程治疗的患者的OS明显优于接受少于12个疗程治疗的患者(中位数:20个月[95%置信区间:12 - 27个月])(中位数:4个月[95%置信区间:1 - 8个月])(p = 0.043)。不良风险细胞遗传学也与较低的1年总生存率相关(33%对69%;p = 0.046)。根据这些结果,并考虑到HMA治疗失败后的不良预后,一旦获得持续缓解,应避免中断HMA治疗。