Giabicani Eloïse, Lemaire Pierre, Brauner Raja
Fondation Ophtalmologique Adolphe de Rothschild, Paris, France.
Université Grenoble Alpes and CNRS, G-SCOP, F-38000 Grenoble, France.
PLoS One. 2015 Apr 2;10(3):e0120588. doi: 10.1371/journal.pone.0120588. eCollection 2015.
It is difficult to determine whether to treat a given girl who has idiopathic central precocious puberty (CPP) with gonadotropin-releasing hormone analog (GnRHa) in terms of adult height (AH). The objective was to provide an easy tool for predicting AH and age at first menstruation at initial evaluation to help guide the decision regarding whether to treat.
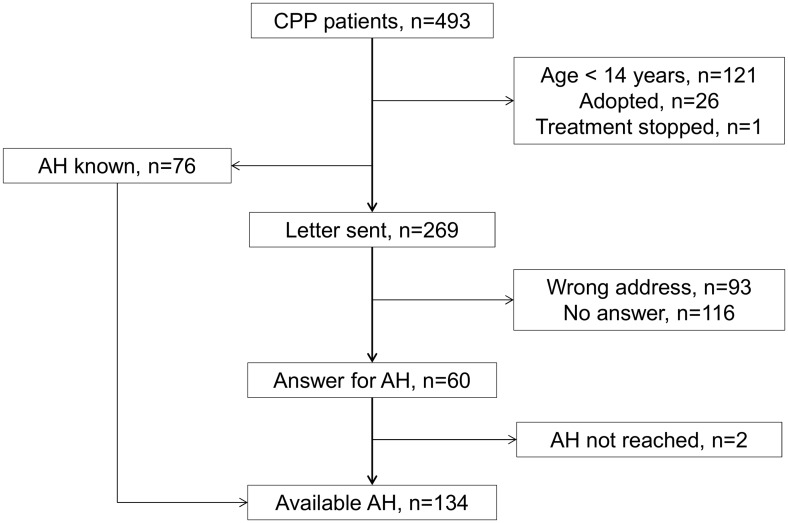
Data analysis using multiple linear regression models was performed in 134 girls with CPP. Among them 78 were given GnRHa because of low predicted AH (n=45), pubertal luteinising hormone (LH)/follicle-stimulating hormone peaks (FSH) ratio (n=50) and/or high plasma estradiol concentration (n=45). 56 girls were followed without treatment.
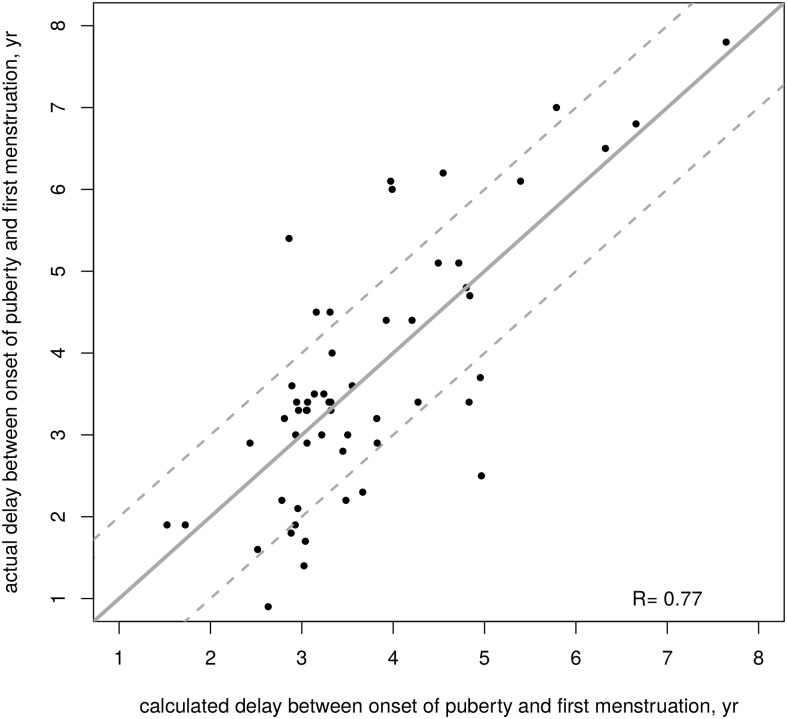
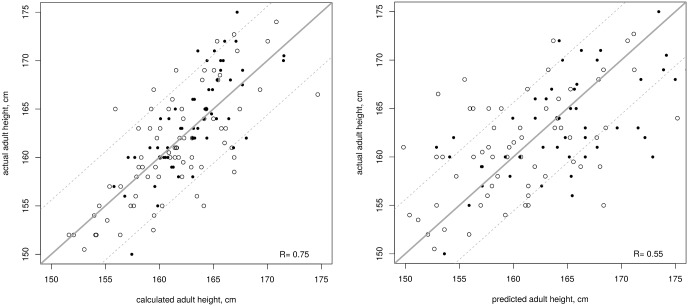
In the whole population, the actual AH (162.1±5.61 cm) was similar to target height (161.7±4.91 cm) and to AH predicted by the Bayley and Pinneau method (161.9±7.98 cm). Separated models for treated and untreated girls provide very close estimations, leading to a unique formula for both groups. The AH (cm) could be calculated at the initial evaluation: 2.21 (height at initial evaluation, SD) + 2.32 (target height, SD) - 1.83 (LH/FSH peaks ratio) + 159.68. The actual AH was lower than the calculated AH by more than 1 SD (5.6 cm) in 11 girls (8.0%). The time between onset of puberty and first menstruation (in untreated girls) can be estimated with: 10.9 - 0.57 (LH/FSH peaks ratio). The formulae are available at http://www.kamick.org/lemaire/med/girls-cpp15.html.
We established formulae that can be used at an initial evaluation to predict the AH, and the time between onset of puberty and first menstruation after spontaneous puberty. The similarity of the formulae for both groups suggests that the treatment had no significant effect on the AH. However, the criteria used to select treatment suggest that it prevents the deterioration of AH in cases with rapidly evolving form of CPP.
就成年身高而言,很难确定对于患有特发性中枢性性早熟(CPP)的特定女孩是否采用促性腺激素释放激素类似物(GnRHa)进行治疗。目的是提供一种简单工具,用于在初始评估时预测成年身高和初潮年龄,以帮助指导治疗决策。
对134例CPP女孩进行了使用多元线性回归模型的数据分析。其中78例因预测成年身高低(n = 45)、青春期促黄体生成素(LH)/促卵泡生成素峰值(FSH)比值(n = 50)和/或血浆雌二醇浓度高(n = 45)而接受GnRHa治疗。56例女孩未接受治疗而进行随访。
在总体人群中,实际成年身高(162.1±5.61厘米)与靶身高(161.7±4.91厘米)以及贝利和皮诺方法预测的成年身高(161.9±7.98厘米)相似。针对接受治疗和未接受治疗女孩的单独模型提供了非常接近的估计值,从而得出了适用于两组的唯一公式。成年身高(厘米)可在初始评估时计算得出:2.21(初始评估时的身高,标准差) + 2.32(靶身高,标准差) - 1.83(LH/FSH峰值比值) + 159.68。11例女孩(8.0%)的实际成年身高比计算得出的成年身高低超过1个标准差(5.6厘米)。青春期开始至初潮的时间(在未接受治疗的女孩中)可用以下公式估计:10.9 - 0.57(LH/FSH峰值比值)。这些公式可在http://www.kamick.org/lemaire/med/girls-cpp15.html获取。
我们建立了可在初始评估时用于预测成年身高以及青春期开始至自然青春期后初潮时间的公式。两组公式的相似性表明治疗对成年身高无显著影响。然而,用于选择治疗的标准表明,在CPP快速进展形式的病例中,它可防止成年身高恶化。