Orthopaedic and Traumatology Department, "G. D'Annunzio" University, Chieti, Italy.
Department of Neurosurgery, "L'Aquila" University, L'Aquila, Italy.
Global Spine J. 2015 Apr;5(2):84-92. doi: 10.1055/s-0034-1395784. Epub 2014 Nov 10.
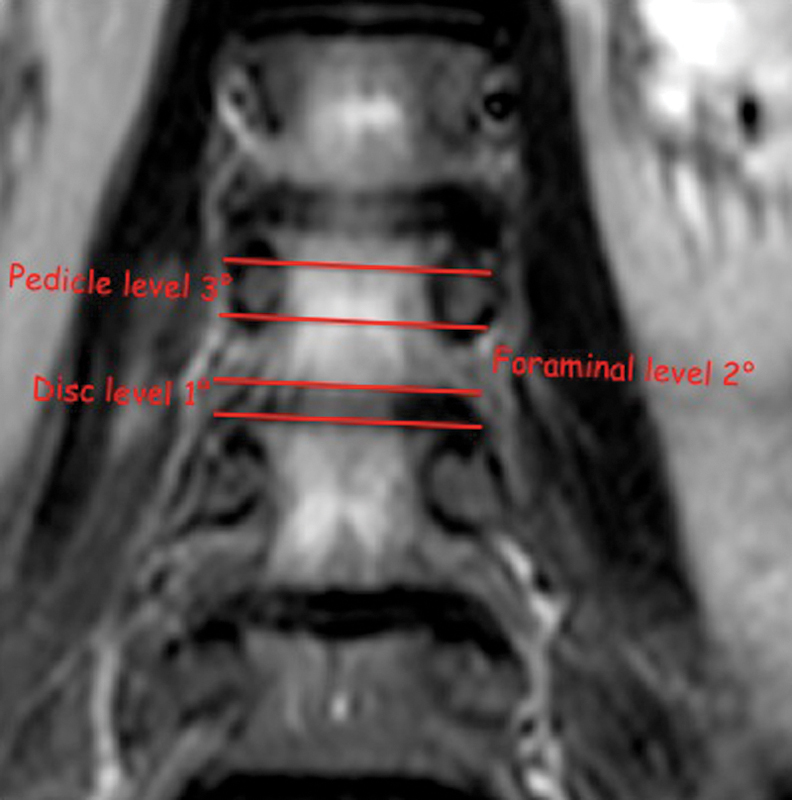
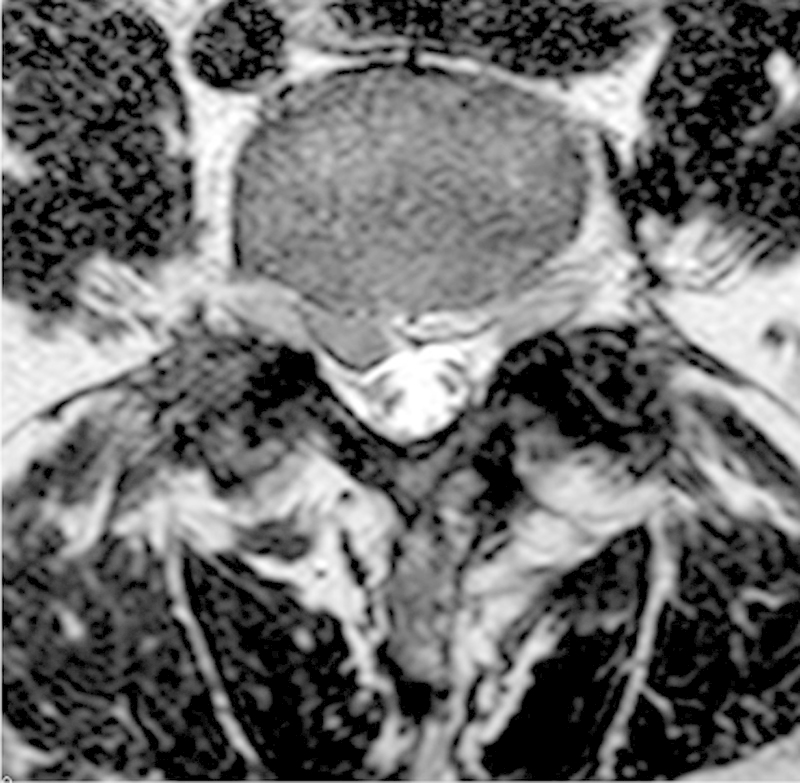
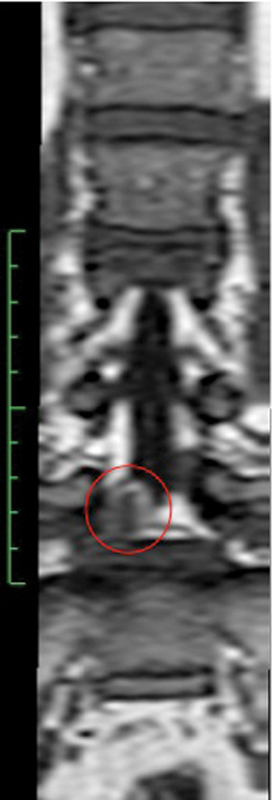
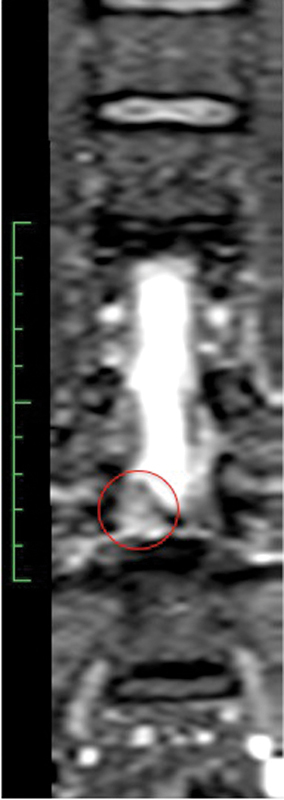
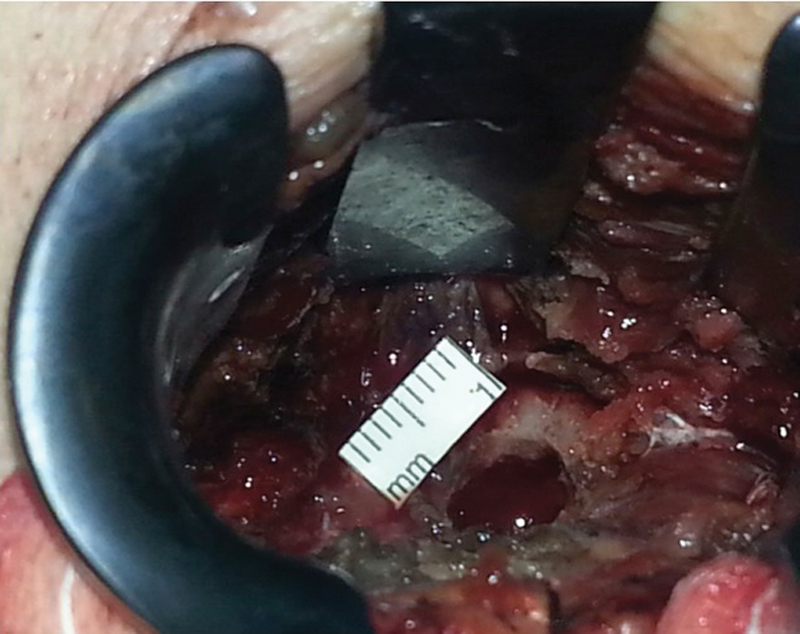
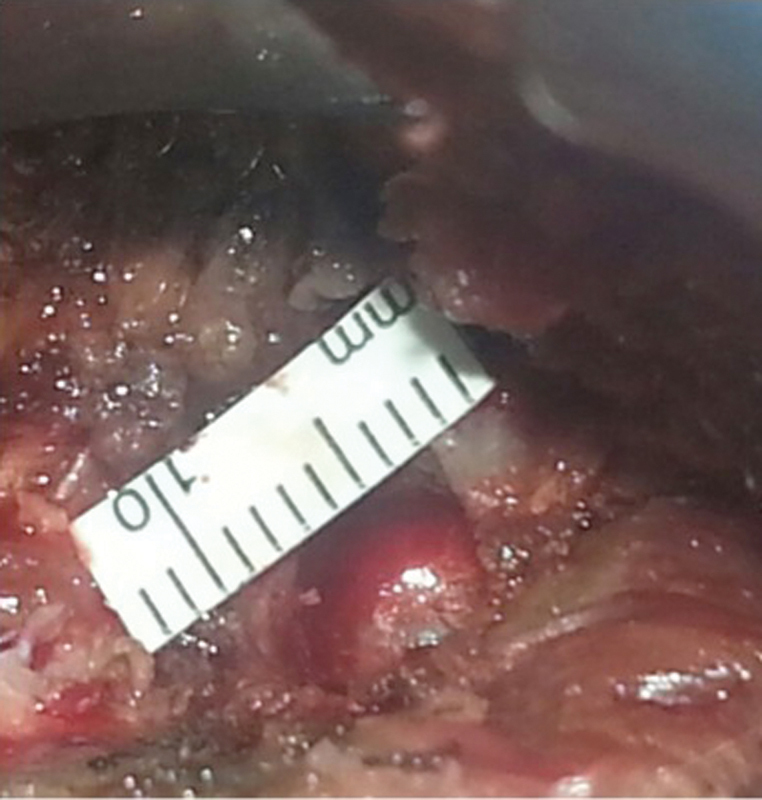
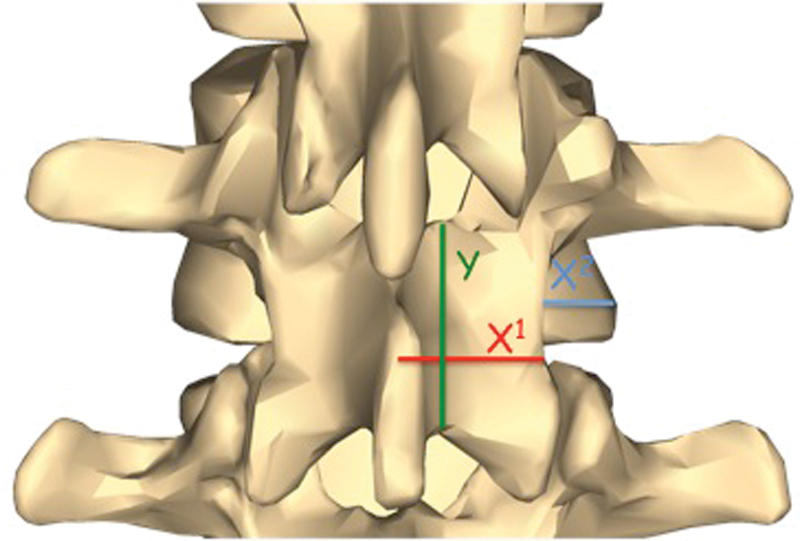
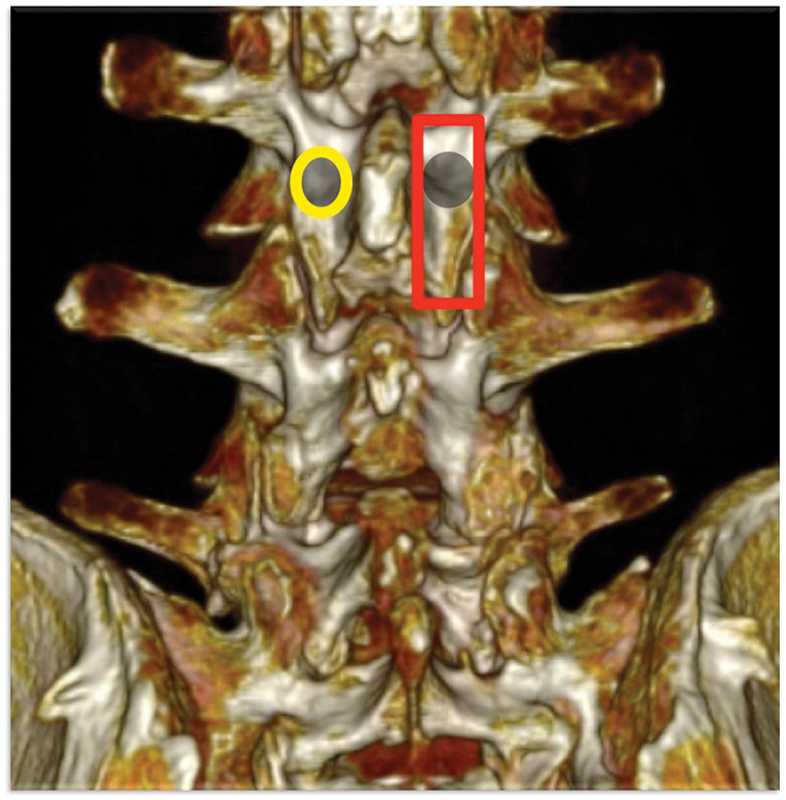
Study Design Retrospective study. Objective The interlaminar approach represents the standard procedure for the surgical treatment of lumbar disk herniation (LDH). In the case of disk herniations in the "hidden zone," it could be necessary to perform laminotomies or laminectomies and partial or total facetectomies to remove the herniated fragment, thus leading to iatrogenic instability. The objective of the study is to evaluate the translaminar approach, in terms of the results, safety, and efficacy compared with the standard approach. Methods Since February 2010, 38 patients (26 men and 12 women; mean age 50.9 years, range 31 to 78 years) with LDH and migration into the hidden zone underwent a microdiskectomy by the translaminar approach. Using a micro-diamond dust-coated burr, a translaminar hole (8 ± 2 mm) was made, with subsequent exposure of the involved root and removal of the fragment. A clinical follow-up was performed at months 1, 3, 6, and 12 using the visual analog scale and the Oswestry Disability Index. All patients were evaluated according to the Spangfort score. Postoperative radiographic evaluations were done at 1, 6, and 12 months (dynamic radiographic studies done at 6 and 12 months). Results In over 60% of cases, L4-L5 was the involved disk. The visualization of the roots was successfully achieved through a translaminar approach. No laminotomies, laminectomies, or partial or total facetectomies were performed. The flavum ligament was always spared. A severe intraoperative bleeding episode occurred in 5% of the cases, due to involvement of the epidural veins, but it did not result in prolonged operative time (mean duration 60 ± 10 minutes). The patients showed a gradual resolution of the back pain and a progressive resolution of the radicular pain and the neurologic deficits. No sign of radiographic instability was documented during the follow-up. No infections, dural tears, or spinal cord injuries occurred. No revision surgery was performed. Conclusion The translaminar approach is the only tissue-sparing technique viable in case of cranially migrated LDH encroaching on the exiting nerve root in the preforaminal zones, for the levels above L2-L3, and in the preforaminal and foraminal zones, for the levels below L3-L4 (L5-S1 included, if a total microdiskectomy is not necessary). The possibility to spare the flavum ligament is one of the main advantages of this technique. According to our experience, the translaminar approach is an effective and safe alternative minimally invasive surgical option.
回顾性研究。目的:层间入路是治疗腰椎间盘突出症(LDH)的标准手术方法。对于“隐藏区”的椎间盘突出,如果要取出突出的碎片,可能需要进行椎板切开术或椎板切除术以及部分或全部关节突切除术,从而导致医源性不稳定。本研究的目的是评估层间入路与标准入路相比在疗效、安全性和有效性方面的情况。方法:自 2010 年 2 月以来,38 例(26 例男性,12 例女性;平均年龄 50.9 岁,范围 31 至 78 岁)患有迁移到隐藏区的 LDH 患者通过层间入路进行微创椎间盘切除术。使用微金刚石粉尘涂层磨头,制作层间孔(8±2mm),随后暴露受累神经根并取出碎片。在术后 1、3、6 和 12 个月使用视觉模拟量表和 Oswestry 残疾指数进行临床随访。所有患者均根据 Spangfort 评分进行评估。术后影像学评估在 1、6 和 12 个月进行(6 和 12 个月进行动态影像学研究)。结果:在超过 60%的病例中,病变位于 L4-L5 椎间盘。通过层间入路成功地实现了神经根的可视化。未进行椎板切开术、椎板切除术、部分或全部关节突切除术。黄韧带始终得以保留。由于硬膜外静脉受累,5%的病例发生严重的术中出血,但未导致手术时间延长(平均手术时间 60±10 分钟)。患者的腰痛逐渐缓解,神经根痛和神经功能缺损逐渐缓解。在随访期间未发现影像学不稳定的迹象。无感染、硬脊膜撕裂或脊髓损伤发生。未行翻修手术。结论:在颅侧迁移的 LDH 侵犯椎间孔出口神经根的情况下,层间入路是唯一可行的保留组织的技术,适用于 L2-L3 以上水平的前孔区和 L3-L4 以下水平的前孔区和椎间孔区(如果不需要进行全微创椎间盘切除术,则包括 L5-S1)。保留黄韧带是该技术的主要优势之一。根据我们的经验,层间入路是一种有效且安全的微创手术替代选择。