Heider Arvela R, Maloney Nancy A, Satchidanand Nikhil, Allen Geoffrey M, Mueller Raymond, Gangloff Steven, Singh Ranjit
Canisius College.
HEALTHeLINK.
EGEMS (Wash DC). 2014 Sep 4;2(3):1089. doi: 10.13063/2327-9214.1089. eCollection 2014.
Disease registries, as part of electronic health records (EHRs), have shown promise in improving care and outcomes. However, little is known about how best to implement them across communities, especially in communities that are not highly integrated. The Western New York (WNY) primary care community consists largely of independent practices using at least 20 different EHR products. This paper discusses the processes undertaken to develop a communitywide EHR disease registry in WNY, improvements it engendered, barriers overcome, and the lessons learned.
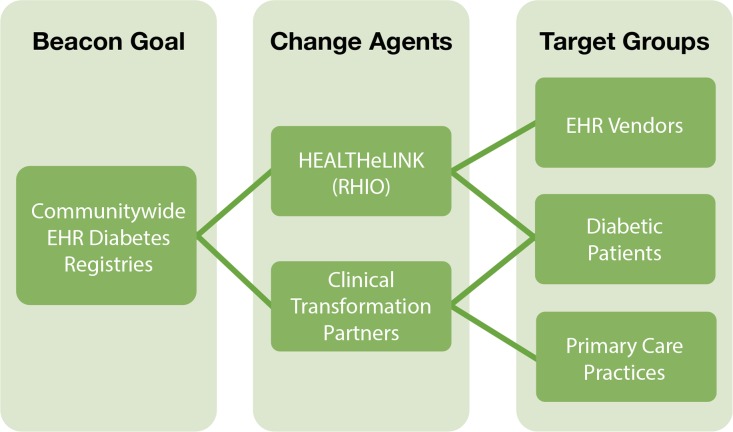
HEALTHeLINK, under the Office of the National Coordinator for Health Information Technology Beacon Community Initiative, reached out to 98 primary care practices in the WNY region to establish EHR-based diabetes registries. Working with practices, community partners, and vendors, registry specifications were created. The registry was piloted with practices using one local vendor's EHR product and then rolled out to other practices, including five other EHR products. Using identified and de-identified registry datasets, quality benchmarking within and between practices and population health management were undertaken.
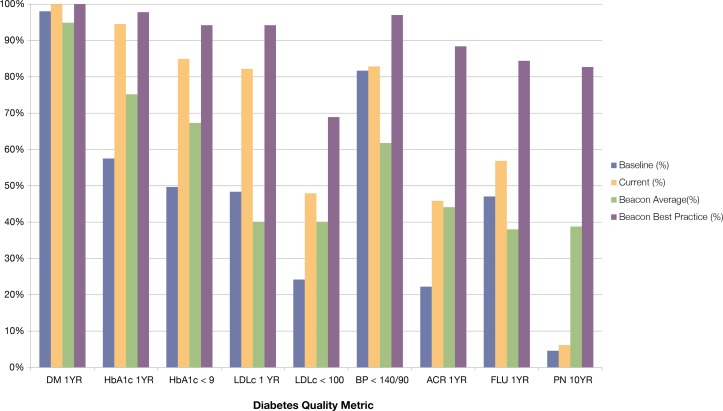
From 2011 to 2013, the WNY Beacon Community assisted 98 practices (344 providers) serving over 50,000 adult diabetic patients. A major focus was on EHR registry development across diverse systems, and overcoming the challenges this presented. The Beacon diabetes registry was implemented at 85 of the 98 targeted practices. Of these registries, 65 met the criteria described in a later section for quality benchmarking and population health management purposes. Practices received quarterly benchmark reports summarizing their performance on key diabetes quality metrics and were compared to community practice averages. Practices used their registries for population health management by identifying and targeting patients in need of follow-up or specific diabetes-related care.
The creation of the registry infrastructure required unified registry technical specifications as well as close collaboration between all parties involved. The WNY experience showed that a useful disease registry can be established in a community largely consisting of numerous disparate primary care practices. This laid the groundwork for the future use of EHR data for a variety of purposes in the community. The methods used and lessons learned through this endeavor may benefit other communities in a similar position, with several disconnected EHRs, to establish unified registries.
疾病登记作为电子健康记录(EHR)的一部分,已显示出改善医疗服务和治疗结果的前景。然而,对于如何在各社区中最佳地实施疾病登记,尤其是在整合程度不高的社区中,人们了解甚少。纽约西部(WNY)的初级医疗社区主要由使用至少20种不同EHR产品的独立医疗机构组成。本文讨论了在WNY开发全社区EHR疾病登记所采取的过程、带来的改进、克服的障碍以及吸取的经验教训。
在卫生信息技术国家协调员办公室的灯塔社区倡议下,HEALTHeLINK联系了WNY地区的98家初级医疗诊所,以建立基于EHR的糖尿病登记系统。与诊所、社区合作伙伴和供应商合作,制定了登记规范。该登记系统在使用一家当地供应商的EHR产品的诊所进行了试点,然后推广到其他诊所,包括其他五种EHR产品。利用已识别和匿名化的登记数据集,在诊所内部和之间进行了质量基准评估以及人群健康管理。
从2011年到2013年,WNY灯塔社区协助了98家诊所(344名医疗服务提供者),为超过50,000名成年糖尿病患者提供服务。主要重点是跨不同系统开发EHR登记系统,并克服由此带来的挑战。在98家目标诊所中的85家实施了灯塔糖尿病登记系统。在这些登记系统中,65家符合后文中所述的用于质量基准评估和人群健康管理目的的标准。诊所收到了季度基准报告,总结了它们在关键糖尿病质量指标上的表现,并与社区诊所的平均水平进行了比较。诊所通过识别和定位需要随访或特定糖尿病相关护理的患者,将其登记系统用于人群健康管理。
创建登记基础设施需要统一的登记技术规范以及所有相关方之间的密切合作。WNY的经验表明,在一个主要由众多不同的初级医疗诊所组成的社区中,可以建立一个有用的疾病登记系统。这为未来在社区中出于各种目的使用EHR数据奠定了基础。通过这项努力所使用的方法和吸取的经验教训可能会使处于类似情况、拥有多个不相连的EHR的其他社区受益,从而建立统一的登记系统。