Danielson Kristin, Beshara Soheir, Qureshi Abdul Rashid, Heimbürger Olof, Lindholm Bengt, Hansson Magnus, Hylander Britta, Germanis Guna, Stenvinkel Peter, Barany Peter
Institution of Laboratory Medicine , Karolinska Institutet , Stockholm , Sweden.
Division of Baxter Novum, CLINTEC, Department of Clinical Science, Intervention and Technology , Karolinska Institutet , Stockholm , Sweden ; Renal Medicine, CLINTEC , Karolinska institutet , Stockholm , Sweden.
Clin Kidney J. 2014 Jun;7(3):275-81. doi: 10.1093/ckj/sfu038. Epub 2014 May 14.
Inflammation impairs erythropoiesis, iron availability and is associated with a higher mortality risk in patients with end-stage renal disease. We studied the associations between Delta-He [the difference between the reticulocyte haemoglobin content (Ret-He) and erythrocyte haemoglobin content], a suggested marker of iron availability, and markers of inflammation, iron status, response to erythropoiesis-stimulating agents (ESAs) and mortality in prevalent peritoneal dialysis (PD) patients.
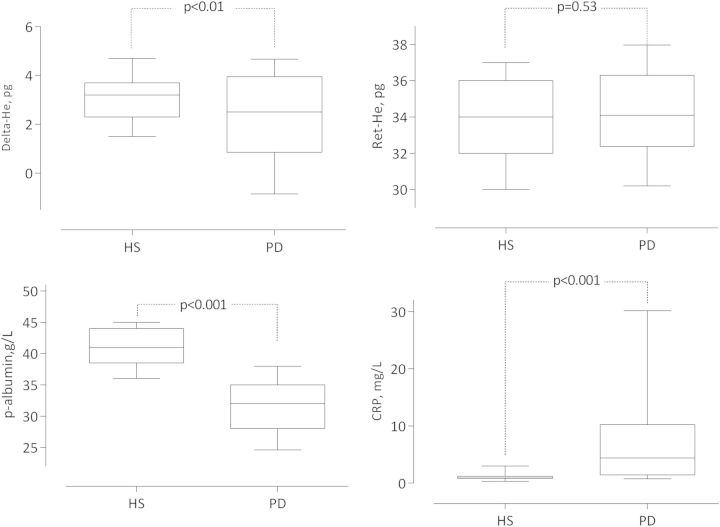
Eighty-two PD patients were followed weekly for 12 weeks with an additional follow-up of 36 months. Delta-He, Ret-He and high-sensitivity C-reactive protein (hs-CRP) were measured weekly and interleukin-6 (IL-6) and iron markers every fourth week. Mortality risk was assessed by Cox proportional hazards model adjusting for potential confounding factors. The relationships between ESA response, inflammatory markers, iron markers and Delta-He were evaluated in the PD patients. The relationship between Delta-He and iron markers was analysed in 87 healthy subjects.
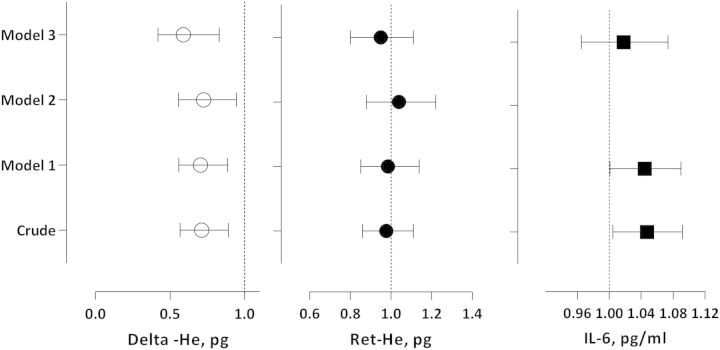
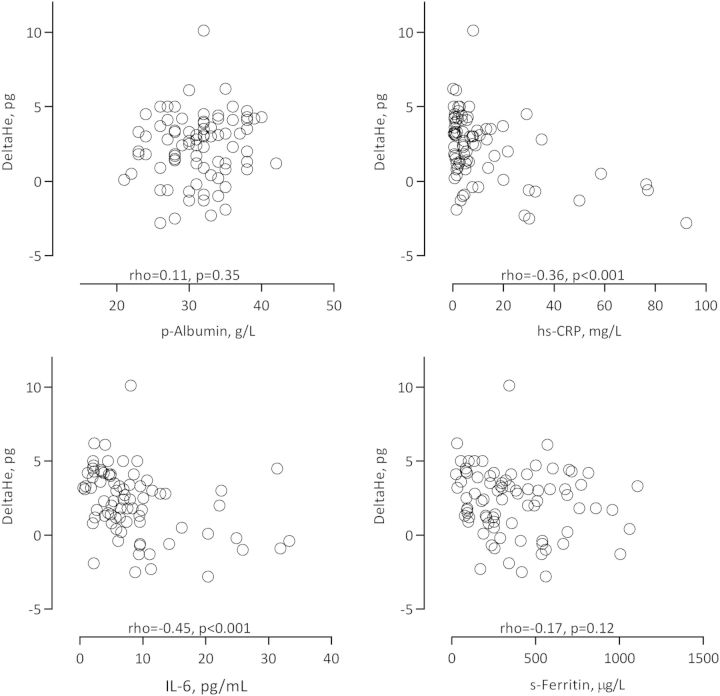
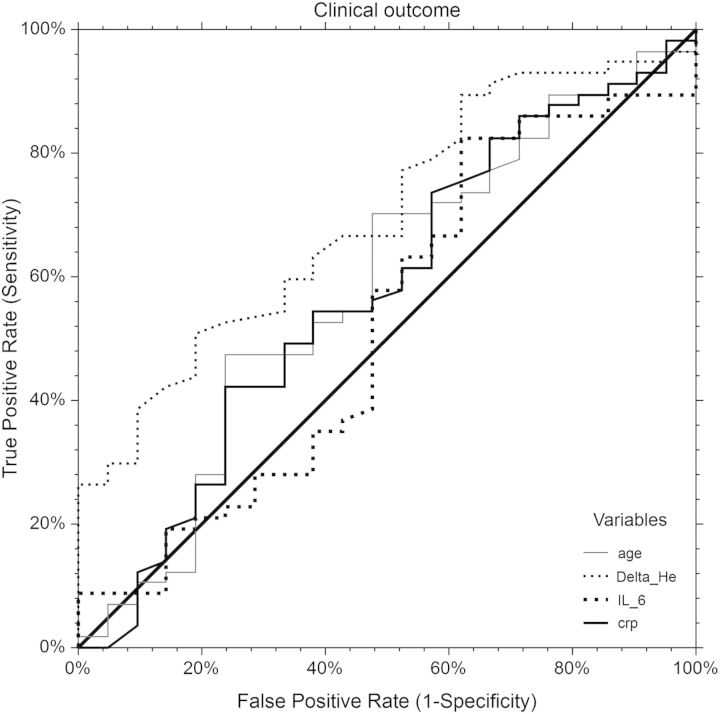
Delta-He correlated with IL-6 (rho = 0.48, P < 0.001), hs-CRP (rho = 0.36, P < 0.001) and ESA hyporesponsivess index (EHRI; rho = -0.44, P < 0.001) in the PD patients. Delta-He did not correlate with iron markers in PD patients nor in healthy subjects. The mean Delta-He levels were significantly different between the tertiles of EHRI (P < 0.01). Delta-He was associated with all-cause mortality risk in PD patients after adjusting for age, gender, hs-CRP, comorbidity and nutritional status [OR 0.70 (0.51-0.96), P < 0.05].
Delta-He independently predicts all-cause mortality in PD patients after adjusting for potential confounders and is a predictor of ESA response in PD patients.
炎症会损害红细胞生成和铁的可用性,并且与终末期肾病患者较高的死亡风险相关。我们研究了作为铁可用性指标的Δ-血红蛋白(网织红细胞血红蛋白含量(Ret-He)与红细胞血红蛋白含量之间的差值)与炎症指标、铁状态、促红细胞生成素(ESA)反应及腹膜透析(PD)患者死亡率之间的关联。
82例PD患者每周随访12周,并额外随访36个月。每周测量Δ-血红蛋白、Ret-He和高敏C反应蛋白(hs-CRP),每四周测量白细胞介素-6(IL-6)和铁指标。通过Cox比例风险模型评估死亡风险,并对潜在混杂因素进行校正。评估PD患者中ESA反应、炎症指标、铁指标与Δ-血红蛋白之间的关系。在87名健康受试者中分析Δ-血红蛋白与铁指标之间的关系。
在PD患者中,Δ-血红蛋白与IL-6(ρ = 0.48,P < 0.001)、hs-CRP(ρ = 0.36,P < 0.001)和ESA低反应指数(EHRI;ρ = -0.44,P < 0.001)相关。在PD患者和健康受试者中,Δ-血红蛋白与铁指标均无相关性。EHRI三分位数之间的平均Δ-血红蛋白水平存在显著差异(P < 0.01)。在对年龄、性别、hs-CRP、合并症和营养状况进行校正后,Δ-血红蛋白与PD患者的全因死亡风险相关[比值比0.70(0.51 - 0.96),P < 0.05]。
校正潜在混杂因素后,Δ-血红蛋白可独立预测PD患者的全因死亡率,并且是PD患者ESA反应的预测指标。