Medical and Nursing Direction, Hospital Clinic de Barcelona. CIBER en Enfermedades Respiratorias (CIBERES), Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Universitat de Barcelona, Barcelona, Spain.
Information System Department, Hospital Clinic de Barcelona, CIBER en Enfermedades Respiratorias (CIBERES), Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Universitat de Barcelona, Barcelona, Spain.
NPJ Prim Care Respir Med. 2015 Apr 9;25:15022. doi: 10.1038/npjpcrm.2015.22.
Chronic obstructive pulmonary disease (COPD) generates a high burden on health care, and hospital admissions represent a substantial proportion of the overall costs of the disease. Integrated care (IC) has shown efficacy to reduce hospitalisations in COPD patients at a pilot level. Deployment strategies for IC services require assessment of effectiveness at the health care system level.
The aim of this study was to explore the effectiveness of a community-based IC service in preventing hospitalisations and emergency department (ED) visits in stable frail COPD patients.
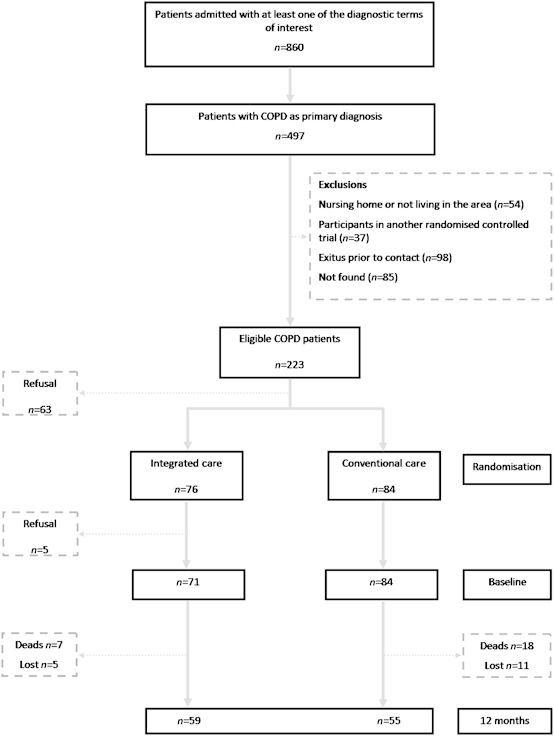
From April to December 2005, 155 frail community-dwelling COPD patients were randomly allocated either to IC (n=76, age 73 (8) years, forced expiratory volume during the first second, FEV1 41(19) % predicted) or usual care (n=84, age 75(9) years, FEV1 44 (20) % predicted) and followed up for 12 months. The IC intervention consisted of the following: (a) patient's empowerment for self-management; (b) an individualised care plan; (c) access to a call centre; and (d) coordination between the levels of care. Thereafter, hospital admissions, ED visits and mortality were monitored for 6 years.
IC enhanced self-management (P=0.02), reduced anxiety-depression (P=0.001) and improved health-related quality of life (P=0.02). IC reduced both ED visits (P=0.02) and mortality (P=0.03) but not hospital admission. No differences between the two groups were seen after 6 years.
The intervention improved clinical outcomes including survival and decreased the ED visits, but it did not reduce hospital admissions. The study facilitated the identification of two key requirements for adoption of IC services in the community: appropriate risk stratification of patients, and preparation of the community-based work force.
慢性阻塞性肺疾病(COPD)给医疗保健带来了沉重负担,住院治疗是该疾病总费用的重要组成部分。初步研究表明,综合护理(IC)可有效降低 COPD 患者的住院率。为了在医疗体系层面评估 IC 服务的实施效果,需要制定部署策略。
本研究旨在探讨基于社区的 IC 服务对稳定期体弱 COPD 患者预防住院和急诊就诊的效果。
2005 年 4 月至 12 月,共纳入 155 例体弱的社区居住 COPD 患者,随机分配至 IC 组(n=76,年龄 73(8)岁,第一秒用力呼气容积占预计值百分比,FEV1 41(19)%)或常规护理组(n=84,年龄 75(9)岁,FEV1 44(20)%),并随访 12 个月。IC 干预措施包括:(a)患者自我管理能力增强;(b)个体化护理计划;(c)获得呼叫中心服务;(d)协调各级医疗服务。之后,监测 6 年内的住院、急诊就诊和死亡率。
IC 增强了患者的自我管理能力(P=0.02),减轻了焦虑抑郁(P=0.001),改善了健康相关生活质量(P=0.02)。IC 降低了急诊就诊(P=0.02)和死亡率(P=0.03),但未降低住院率。6 年后两组间无差异。
该干预措施改善了临床结局,包括生存率,降低了急诊就诊率,但未降低住院率。本研究确定了在社区中采用 IC 服务的两个关键要求:对患者进行适当的风险分层,以及对社区工作人员进行培训。