Leibson Cynthia L, Long Kirsten Hall, Ransom Jeanine E, Roberts Rosebud O, Hass Steven L, Duhig Amy M, Smith Carin Y, Emerson Jane A, Pankratz V Shane, Petersen Ronald C
Department of Health Sciences Research, Mayo Clinic, Rochester, MN, USA.
K Long Health Economics Consulting LLC, St. Paul, MN, USA.
Alzheimers Dement. 2015 Aug;11(8):917-32. doi: 10.1016/j.jalz.2015.01.007. Epub 2015 Apr 6.
Objective cost estimates and source of cost differences are needed across the spectrum of cognition, including cognitively normal (CN), mild cognitive impairment (MCI), newly discovered dementia, and prevalent dementia.
Subjects were a subset of the Mayo Clinic Study of Aging stratified-random sampling of Olmsted County, MN, residents aged 70 to 89 years. A neurologist reviewed provider-linked medical records to identify prevalent dementia (review date = index). Remaining subjects were invited to participate in prospective clinical/neuropsychological assessments; participants were categorized as CN, MCI, or newly discovered dementia (assessment date = index). Costs for medical services/procedures 1-year pre-index (excluding indirect and long-term care costs) were estimated using line-item provider-linked administrative data. We estimated contributions of care-delivery site and comorbid conditions (including and excluding neuropsychiatric diagnoses) to between-category cost differences.
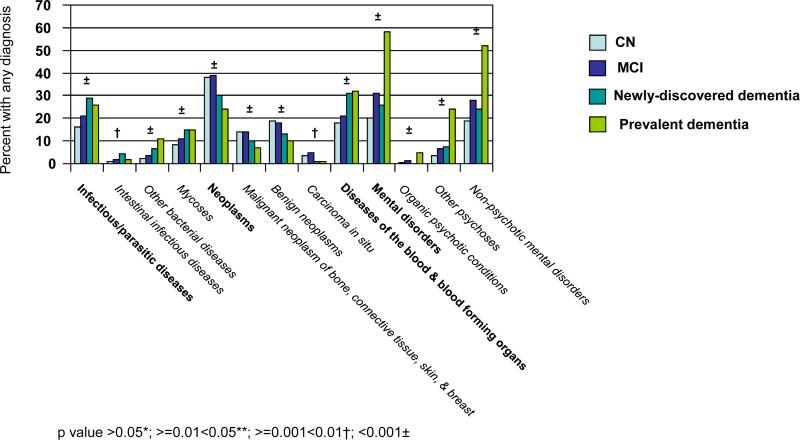
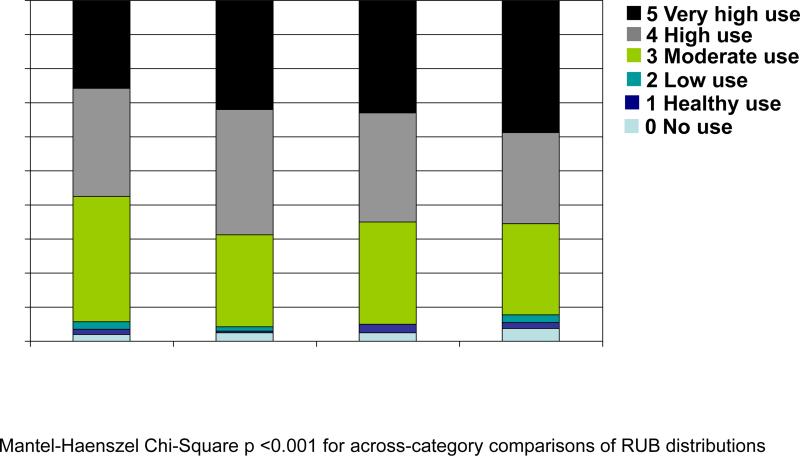
Annual mean medical costs for CN, MCI, newly discovered dementia, and prevalent dementia were $6042, $6784, $9431, $11,678, respectively. Hospital inpatient costs contributed 70% of total costs for prevalent dementia and accounted for differences between CN and both prevalent and newly discovered dementia. Ambulatory costs accounted for differences between CN and MCI. Age-, sex-, education-adjusted differences reached significance for CN versus newly discovered and prevalent dementia and for MCI versus prevalent dementia. After considering all comorbid diagnoses, between-category differences were reduced (e.g., prevalent dementia minus MCI (from $4842 to $3575); newly discovered dementia minus CN (from $3578 to $711)). Following the exclusion of neuropsychiatric diagnoses from comorbidity adjustment, between-category differences tended to revert to greater differences.
Cost estimates did not differ significantly between CN and MCI. Substantial differences between MCI and prevalent dementia reflected high inpatient costs for dementia and appear partly related to co-occurring mental disorders. Such comparisons can help inform models aimed at identifying where, when, and for which individuals proposed interventions might be cost-effective.
需要对认知谱范围内的客观成本估计及成本差异来源进行评估,认知谱包括认知正常(CN)、轻度认知障碍(MCI)、新发现的痴呆症以及患痴呆症。
研究对象是梅奥诊所衰老研究的一个子集,对明尼苏达州奥尔姆斯特德县70至89岁居民进行分层随机抽样。神经科医生查阅与医疗服务提供者相关的病历,以确定患痴呆症情况(审查日期 = 索引日期)。其余受试者受邀参加前瞻性临床/神经心理学评估;参与者被分类为CN、MCI或新发现的痴呆症(评估日期 = 索引日期)。使用与医疗服务提供者相关的明细行政数据估算索引日期前1年的医疗服务/程序成本(不包括间接和长期护理成本)。我们估计了医疗服务提供地点和共病情况(包括和不包括神经精神疾病诊断)对类别间成本差异的影响。
CN、MCI、新发现的痴呆症和患痴呆症的年均医疗成本分别为6042美元、6784美元、9431美元和11,678美元。住院患者成本占患痴呆症总成本的70%,是CN与患痴呆症及新发现的痴呆症之间成本差异的原因。门诊成本是CN与MCI之间成本差异的原因。年龄、性别、教育程度调整后的差异在CN与新发现的痴呆症及患痴呆症之间以及MCI与患痴呆症之间具有统计学意义。在考虑所有共病诊断后,类别间差异有所减少(例如,患痴呆症减去MCI(从4842美元降至3575美元);新发现的痴呆症减去CN(从3578美元降至711美元))。在共病调整中排除神经精神疾病诊断后,类别间差异往往又恢复到更大的差异。
CN和MCI之间的成本估计没有显著差异。MCI和患痴呆症之间的巨大差异反映了痴呆症患者的高住院成本,并且似乎部分与并发的精神障碍有关。此类比较有助于为旨在确定在何处、何时以及针对哪些个体进行干预可能具有成本效益的模型提供信息。