de Lange Marit M A, Hukkelhoven Chantal W P M, Munster Janna M, Schneeberger Peter M, van der Hoek Wim
Centre for Infectious Disease Control, National Institute for Public Health and the Environment (RIVM), Bilthoven, the Netherlands.
The Netherlands Perinatal Registry, Utrecht, the Netherlands.
BMJ Open. 2015 Apr 10;5(4):e006821. doi: 10.1136/bmjopen-2014-006821.
Whether areas affected by Q fever during a large outbreak (2008-2010) had higher rates of adverse pregnancy outcomes than areas not affected by Q fever.
Nationwide registry-based ecological study.
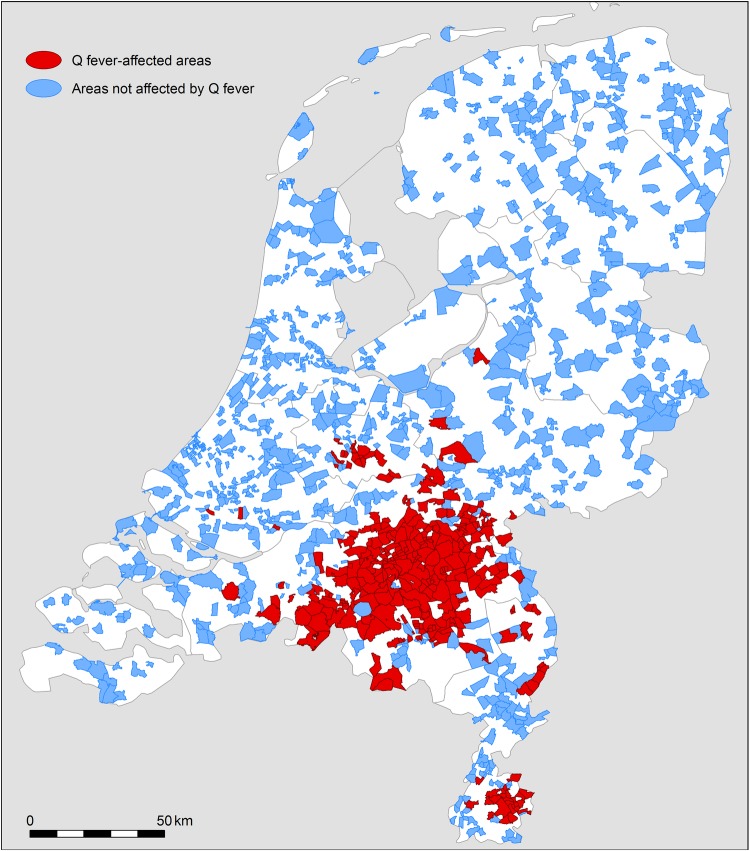
Pregnant women in areas affected and not affected by Q fever in the Netherlands, 2003-2004 and 2008-2010.
Index group (N=58,737): pregnant women in 307 areas with more than two Q fever notifications. Reference group (N=310,635): pregnant women in 921 areas without Q fever notifications. As a baseline, pregnant women in index and reference areas in the years 2003-2004 were also included in the reference group to estimate the effect of Q fever in 2008-2010, and not the already existing differences before the outbreak.
Preterm delivery, small for gestational age, perinatal mortality.
In 2008-2010, there was no association between residing in a Q fever-affected area and both preterm delivery (adjusted OR 1.01 (95% CI 0.94 to 1.08)), and perinatal mortality (adjusted OR 0.87 (95% CI 0.72 to 1.05)). In contrast, we found a weak significant association between residing in a Q fever-affected area in 2008-2010 and small for gestational age (adjusted OR 1.06 (95% CI 1.01 to 1.12)), with a population-attributable fraction of 0.70% (95% CI 0.07% to 1.34%). We observed no dose-response relation for this outcome with increasing Q fever notifications, and we did not find a stronger association for women who were in their first trimester of pregnancy during the months of high human Q fever incidence.
This study found a weak association between residing in a Q fever-affected area and the pregnancy outcome small for gestational age. Early detection of infection would require mass screening of pregnant women; this does not seem to be justified considering these results, and the uncertainties about its efficacy and the adverse effects of antibiotic treatment.
在一次大规模疫情(2008 - 2010年)期间,受Q热影响的地区不良妊娠结局发生率是否高于未受Q热影响的地区。
基于全国登记处的生态学研究。
2003 - 2004年和2008 - 2010年荷兰受Q热影响和未受Q热影响地区的孕妇。
索引组(N = 58,737):307个有超过两例Q热报告地区的孕妇。参照组(N = 310,635):921个无Q热报告地区的孕妇。作为基线,2003 - 2004年索引地区和参照地区的孕妇也纳入参照组,以评估2008 - 2010年Q热的影响,而非疫情爆发前已存在的差异。
早产、小于胎龄儿、围产儿死亡率。
在2008 - 2010年,居住在受Q热影响地区与早产(校正比值比1.01(95%可信区间0.94至1.08))和围产儿死亡率(校正比值比0.87(95%可信区间0.72至1.05))均无关联。相比之下,我们发现2008 - 2010年居住在受Q热影响地区与小于胎龄儿之间存在微弱的显著关联(校正比值比1.06(95%可信区间1.01至1.12)),人群归因分数为0.70%(95%可信区间0.07%至1.34%)。对于这一结局,我们未观察到随着Q热报告数量增加的剂量反应关系,并且对于在人类Q热高发月份处于妊娠早期的女性,未发现更强的关联。
本研究发现居住在受Q热影响地区与小于胎龄儿这一妊娠结局之间存在微弱关联。早期感染检测需要对孕妇进行大规模筛查;考虑到这些结果以及抗生素治疗的疗效和不良反应的不确定性,这样做似乎没有道理。