O'Dwyer Ralph Hurley, Acosta Andrés, Camilleri Michael, Burton Duane, Busciglio Irene, Bharucha Adil E
Clinical Enteric Neuroscience Translational and Epidemiological Research (C.E.N.T.E.R.), Division of Gastroenterology and Hepatology, Mayo Clinic, Charlton Bldg., Rm. 8-110, 200 First St. S.W., Rochester, MN, 55905, USA,
Dig Dis Sci. 2015 Aug;60(8):2398-407. doi: 10.1007/s10620-015-3645-5. Epub 2015 Apr 14.
Chronic megacolon is a rare disease of the colonic motor function characterized by a permanent increase in colonic diameter.
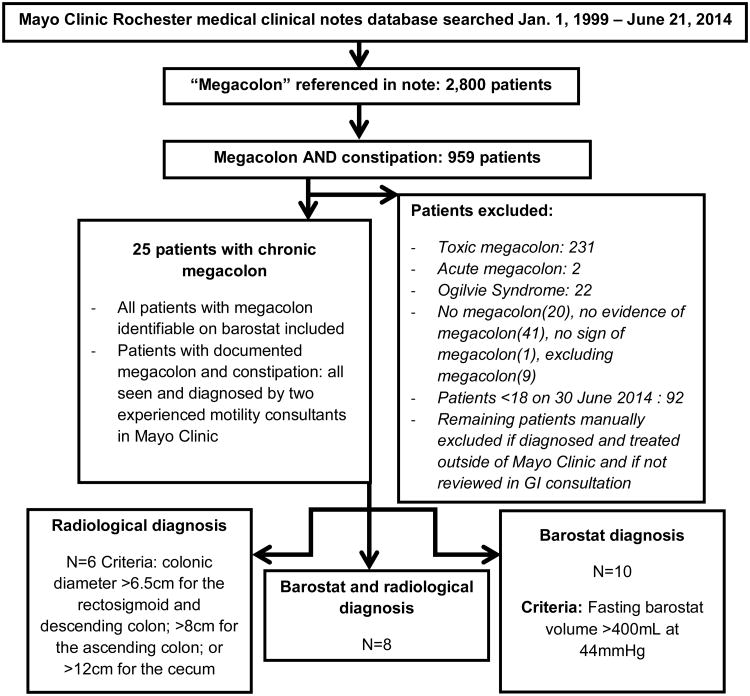
We reviewed electronic medical records of all patients diagnosed with chronic megacolon from 1999 to 2014 at Mayo Clinic. Our aim was to summarize clinical and motility features, including colonic compliance and tone measured by colonic barostat-controlled 10-cm-long infinitely compliant balloon. Colonic compliance curves were compared to healthy control (40) and disease (47) control groups.
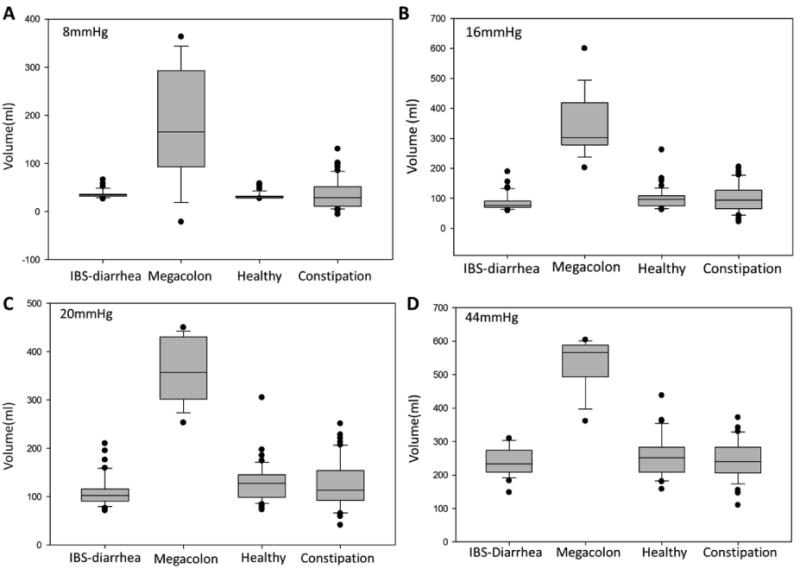
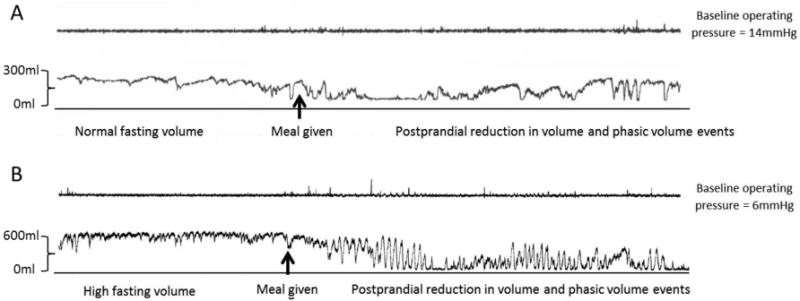
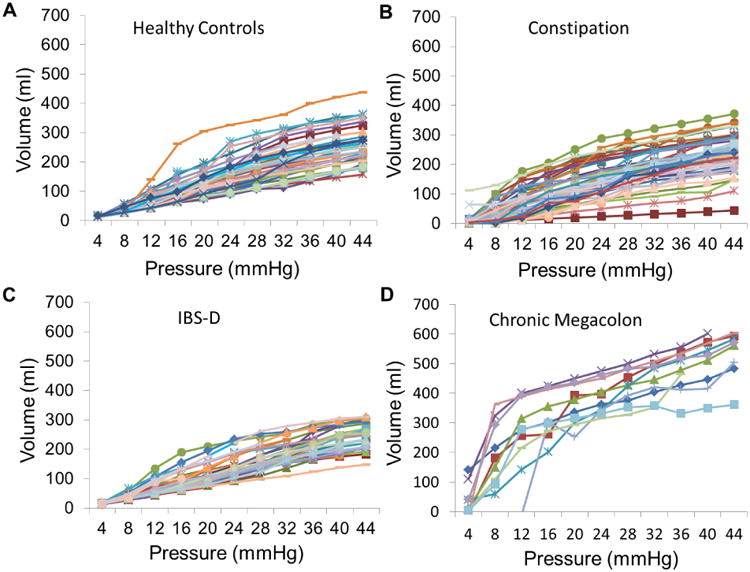
Among 24 identified patients, the mean maximal colonic diameter on abdominal radiograph was 12.7 ± 0.8 cm. The cause of megacolon was idiopathic in 16 of 24 and secondary in 8 of 24. A relatively high prevalence (10/24) of comorbid pelvic floor dyssynergia was identified. At the time of this report, 16 patients had undergone colectomy. In general, megacolon presented high fasting colonic volume at relatively low pressures (16-20 mmHg), suggesting high colonic compliance; similarly, volumes at operating pressures that ensured apposition of the balloon to the colonic wall suggested low colonic tone. Median balloon volume at 44 mmHg distension was 584 mL (IQR 556.5-600) in patients with megacolon compared to 251 mL (212-281) in healthy, 240 mL (207-286) in functional constipation, and 241 mL (210.8-277.5) in diarrhea-predominant irritable bowel syndrome controls. Colon's tonic response to feeding was generally intact, and there was frequently maintained phasic contractile response to feeding.
Chronic megacolon is a severe colonic dysmotility, manifesting radiologically with increased colonic diameter; it can be proven by measuring colonic compliance and typically requires colectomy because of failed medical therapy.
慢性巨结肠是一种罕见的结肠运动功能疾病,其特征为结肠直径永久性增大。
我们回顾了1999年至2014年在梅奥诊所诊断为慢性巨结肠的所有患者的电子病历。我们的目的是总结临床和动力特征,包括通过结肠压力测定仪控制的10厘米长无限顺应性球囊测量的结肠顺应性和张力。将结肠顺应性曲线与健康对照组(40例)和疾病对照组(47例)进行比较。
在24例确诊患者中,腹部X线片上结肠的平均最大直径为12.7±0.8厘米。24例中16例巨结肠病因不明,8例为继发性。共发现相对较高比例(10/24)的合并盆底功能失调。在本报告发布时,16例患者已接受结肠切除术。一般来说,巨结肠在相对较低压力(16 - 20毫米汞柱)下空腹结肠容积较高,提示结肠顺应性高;同样,在确保球囊与结肠壁贴合的操作压力下的容积提示结肠张力低。巨结肠患者在44毫米汞柱扩张时球囊容积中位数为584毫升(四分位间距556.5 - 600),而健康对照组为251毫升(212 - 281),功能性便秘组为240毫升(207 - 286),腹泻型肠易激综合征对照组为241毫升(210.8 - 277.5)。结肠对进食的紧张性反应通常完好无损,并且对进食经常保持阶段性收缩反应。
慢性巨结肠是一种严重的结肠动力障碍,在影像学上表现为结肠直径增大;可通过测量结肠顺应性来证实,由于药物治疗无效,通常需要进行结肠切除术。