Naseef Abdulrahman, Behr Elijah R, Batchvarov Velislav N
Center for Health Studies, Prince Sultan Military Medical City, Riyadh, Saudi Arabia ; Cardiac and Vascular Sciences Research Centre, St. George's University of London, London, United Kingdom.
Cardiac and Vascular Sciences Research Centre, St. George's University of London, London, United Kingdom.
J Saudi Heart Assoc. 2015 Apr;27(2):96-108. doi: 10.1016/j.jsha.2014.06.004. Epub 2014 Jul 3.
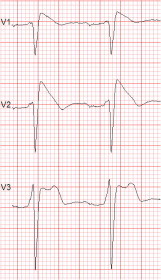
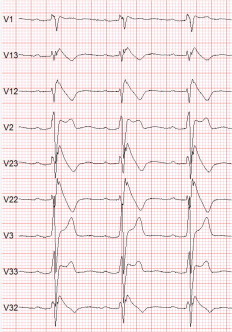
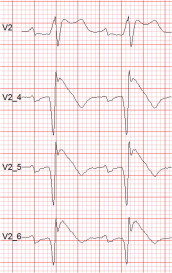
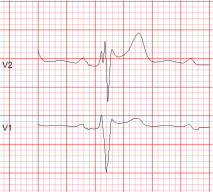
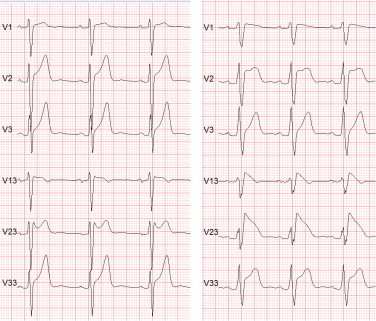
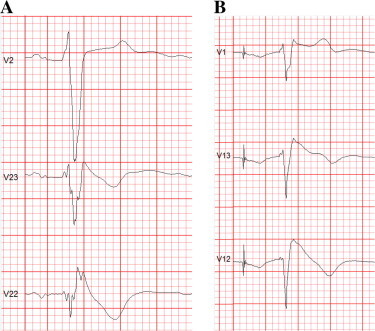
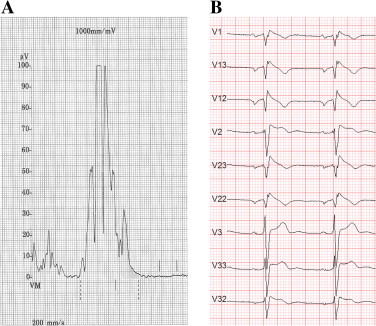
The Brugada syndrome (BrS) is a malignant, genetically-determined, arrhythmic syndrome manifesting as syncope or sudden cardiac death (SCD) in individuals with structurally normal hearts. The diagnosis of the BrS is mainly based on the presence of a spontaneous or Na + channel blocker induced characteristic, electrocardiographic (ECG) pattern (type 1 or coved Brugada ECG pattern) typically seen in leads V1 and V2 recorded from the 4th to 2nd intercostal (i.c.) spaces. This pattern needs to be distinguished from similar ECG changes due to other causes (Brugada ECG phenocopies). This review focuses mainly on the ECG-based methods for diagnosis and arrhythmia risk assessment in the BrS. Presently, the main unresolved clinical problem is the identification of those patients at high risk of SCD who need implantable cardioverter-defibrillator (ICD), which is the only therapy with proven efficacy. Current guidelines recommend ICD implantation only in patients with spontaneous type 1 ECG pattern, and either history of aborted cardiac arrest or documented sustained VT (class I), or syncope of arrhythmic origin (class IIa) because they are at high risk of recurrent arrhythmic events (up to 10% or more annually for those with aborted cardiac arrest). The majority of BrS patients are asymptomatic when diagnosed and considered to have low risk (around 0.5% annually) and therefore not indicated for ICD. The majority of SCD victims in the BrS, however, had no symptoms prior to the fatal event and therefore were not protected with an ICD. While some ECG markers such as QRS fragmentation, infero-lateral early repolarisation, and abnormal late potentials on signal-averaged ECG are known to be linked to increased arrhythmic risk, they are not sufficiently sensitive or specific. Potential novel ECG-based strategies for risk stratification are discussed based on computerised methods for depolarisation and repolarisation analysis, a composite approach targeting several major components of ventricular arrhythmogenesis, and the collection of large digital ECG databases in genotyped BrS patients and their relatives.
Brugada综合征(BrS)是一种恶性的、由基因决定的心律失常综合征,在心脏结构正常的个体中表现为晕厥或心脏性猝死(SCD)。BrS的诊断主要基于自发出现或由钠通道阻滞剂诱发的特征性心电图(ECG)模式(1型或穹窿型Brugada心电图模式),通常见于第4至第2肋间(i.c.)间隙记录的V1和V2导联。这种模式需要与其他原因导致的类似ECG变化(Brugada心电图拟表型)相鉴别。本综述主要关注基于ECG的BrS诊断方法和心律失常风险评估。目前,主要未解决的临床问题是识别那些有SCD高风险且需要植入式心律转复除颤器(ICD)的患者,ICD是唯一经证实有效的治疗方法。当前指南建议仅在有自发1型ECG模式且有心脏骤停复苏史或记录到持续性室性心动过速(VT)(I类),或心律失常性晕厥(IIa类)的患者中植入ICD,因为他们有较高的心律失常复发风险(心脏骤停复苏者每年高达10%或更高)。大多数BrS患者在诊断时无症状,被认为风险较低(每年约0.5%),因此不适合植入ICD。然而,BrS中大多数SCD受害者在致命事件发生前没有症状,因此未受到ICD的保护。虽然一些ECG标志物如QRS波碎裂、下侧壁早期复极以及信号平均心电图上的异常晚期电位已知与心律失常风险增加有关,但它们的敏感性或特异性不足。基于去极化和复极化分析的计算机化方法、针对室性心律失常发生的几个主要成分的综合方法以及在基因分型的BrS患者及其亲属中收集大型数字ECG数据库,讨论了基于ECG的潜在新的风险分层策略。