Gewandter Jennifer S, Dworkin Robert H, Turk Dennis C, Farrar John T, Fillingim Roger B, Gilron Ian, Markman John D, Oaklander Anne Louise, Polydefkis Michael J, Raja Srinivasa N, Robinson James P, Woolf Clifford J, Ziegler Dan, Ashburn Michael A, Burke Laurie B, Cowan Penney, George Steven Z, Goli Veeraindar, Graff Ole X, Iyengar Smriti, Jay Gary W, Katz Joel, Kehlet Henrik, Kitt Rachel A, Kopecky Ernest A, Malamut Richard, McDermott Michael P, Palmer Pamela, Rappaport Bob A, Rauschkolb Christine, Steigerwald Ilona, Tobias Jeffrey, Walco Gary A
Department of Anesthesiology, University of Rochester, Rochester, NY, USA University of Washington, Seattle, WA, USA University of Pennsylvania, Philadelphia, PA, USA University of Florida, Gainesville, FL, USA Queen's University, Kingston, ON, Canada Harvard University, Boston, MS, USA Johns Hopkins University, Baltimore, MD, USA German Diabetes Center at Heinrich Heine University, Düsseldorf, Germany Lora Group, LLC, Royal Oak, MD, USA American Chronic Pain Association, Rocklin, CA, USA Pfizer and Duke University, Raleigh-Duram, NC, USA GlaxoSmithKline, London, United Kingdom Eli Lilly, Indianapolis, IN, USA Virtuous Pharma, Inc, Raleigh-Durham, NC, USA York University, Toronto, ON, Canada Rigshospitalet, Copenhagen University, Denmark Endo Pharmaceuticals, Inc, Malvern, PA, USA Teva Pharmaceuticals, North Wales, PA, USA AcelRx, Redwood City, CA, USA Arlington, VA, USA Johnson and Johnson, Titusville, NJ, USA Grünenthal GMbH, Aachen, Germany Jazz Pharmaceuticals, Palo Alto, CA, USA.
Pain. 2015 Jul;156(7):1184-1197. doi: 10.1097/j.pain.0000000000000191.
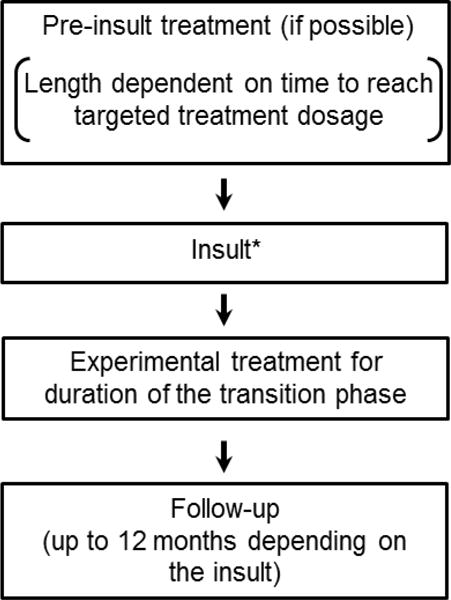
Although certain risk factors can identify individuals who are most likely to develop chronic pain, few interventions to prevent chronic pain have been identified. To facilitate the identification of preventive interventions, an IMMPACT meeting was convened to discuss research design considerations for clinical trials investigating the prevention of chronic pain. We present general design considerations for prevention trials in populations that are at relatively high risk for developing chronic pain. Specific design considerations included subject identification, timing and duration of treatment, outcomes, timing of assessment, and adjusting for risk factors in the analyses. We provide a detailed examination of 4 models of chronic pain prevention (ie, chronic postsurgical pain, postherpetic neuralgia, chronic low back pain, and painful chemotherapy-induced peripheral neuropathy). The issues discussed can, in many instances, be extrapolated to other chronic pain conditions. These examples were selected because they are representative models of primary and secondary prevention, reflect persistent pain resulting from multiple insults (ie, surgery, viral infection, injury, and toxic or noxious element exposure), and are chronically painful conditions that are treated with a range of interventions. Improvements in the design of chronic pain prevention trials could improve assay sensitivity and thus accelerate the identification of efficacious interventions. Such interventions would have the potential to reduce the prevalence of chronic pain in the population. Additionally, standardization of outcomes in prevention clinical trials will facilitate meta-analyses and systematic reviews and improve detection of preventive strategies emerging from clinical trials.
尽管某些风险因素能够识别出最有可能发展为慢性疼痛的个体,但已确定的预防慢性疼痛的干预措施却很少。为推动预防干预措施的识别,召开了一次IMMPACT会议,以讨论针对调查慢性疼痛预防的临床试验的研究设计考量因素。我们介绍了针对处于慢性疼痛较高发病风险人群的预防试验的一般设计考量因素。具体设计考量因素包括受试者识别、治疗的时机和持续时间、结局、评估时机以及在分析中对风险因素进行调整。我们详细审视了4种慢性疼痛预防模型(即慢性术后疼痛、带状疱疹后神经痛、慢性下腰痛以及化疗引起的疼痛性周围神经病变)。在许多情况下,所讨论的问题可外推至其他慢性疼痛病症。选择这些例子是因为它们是一级和二级预防的代表性模型,反映了由多种损伤(即手术、病毒感染、损伤以及接触有毒或有害物质)导致的持续性疼痛,并且是采用一系列干预措施进行治疗的慢性疼痛病症。慢性疼痛预防试验设计的改进可提高试验灵敏度,从而加速有效干预措施的识别。此类干预措施有可能降低人群中慢性疼痛的患病率。此外,预防临床试验结局的标准化将有助于进行荟萃分析和系统评价,并改善对临床试验中出现的预防策略的检测。