Cooper Timothy, Biron Vincent L, Fast David, Tam Raymond, Carey Thomas, Shmulevitz Maya, Seikaly Hadi
Division of Otolaryngology - Head and Neck Surgery, Department of Surgery, University of Alberta, 1E4 University of Alberta Hospital, 1E4 Walter Mackenzie Center, 8440 112 St., Edmonton, AB, T6G 2B7, Canada.
Faculty of Science 1-001 CCIS, University of Alberta, Edmonton, AB, T6G 2E9, Canada.
J Otolaryngol Head Neck Surg. 2015 Feb 24;44(1):8. doi: 10.1186/s40463-015-0062-x.
The management of patients with advanced stages of head and neck cancer requires a multidisciplinary and multimodality treatment approach which includes a combination of surgery, radiation, and chemotherapy. These toxic treatment protocols have significantly improved survival outcomes in a distinct population of human papillomavirus (HPV) associated oropharyngeal cancer. HPV negative head and neck squamous cell carcinoma (HNSCC) remains a challenge to treat because there is only a modest improvement in survival with the present treatment regimens, requiring innovative and new treatment approaches. Oncolytic viruses used as low toxicity adjunct cancer therapies are novel, potentially effective treatments for HNSCC. One such oncolytic virus is Respiratory Orphan Enteric virus or reovirus. Susceptibility of HNSCC cells towards reovirus infection and reovirus-induced cell death has been previously demonstrated but has not been compared in HPV positive and negative HNSCC cell lines.
To compare the infectivity and oncolytic activity of reovirus in HPV positive and negative HNSCC cell lines.
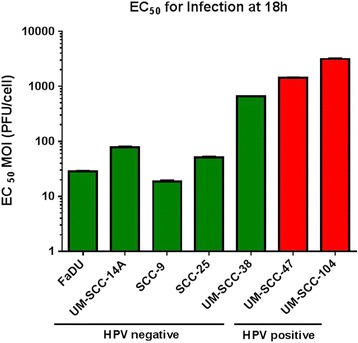
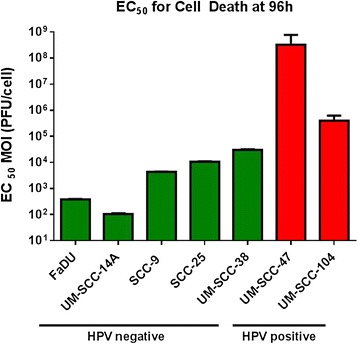
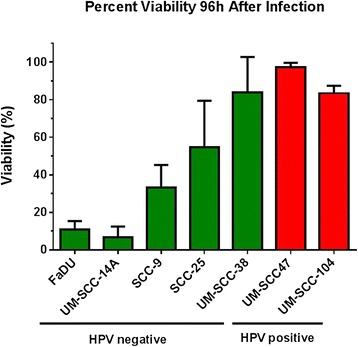
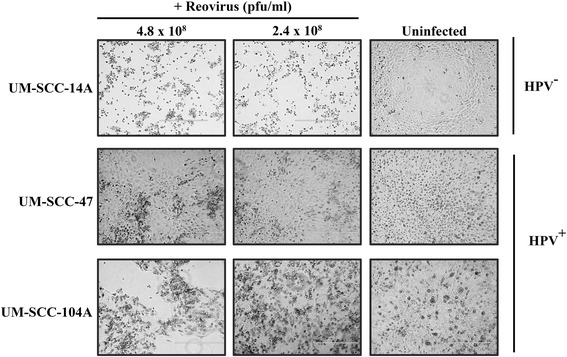
Seven HNSCC cell lines were infected with serial dilutions of reovirus. Two cell lines (UM-SCC-47 and UM-SCC-104) were positive for type 16 HPV. Infectivity was measured using a cell-based ELISA assay 18 h after infection. Oncolytic activity was determined using an alamar blue viability assay 96 h after infection. Non-linear regression models were used to calculate the amounts of virus required to infect and to cause cell death in 50% of a given cell line (EC50). EC50 values were compared.
HPV negative cells were more susceptible to viral infection and oncolysis compared to HPV positive cell lines. EC50 for infectivity at 18 h ranged from multiplicity of infection (MOI) values (PFU/cell) of 18.6 (SCC-9) to 3133 (UM-SCC 104). EC50 for cell death at 96 h ranged from a MOI (PFU/cell) of 1.02×10(2) (UM-SCC-14A) to 3.19×10(8) (UM-SCC-47). There was a 3×10(6) fold difference between the least susceptible cell line (UM-SCC-47) and the most susceptible line (UM-SCC 14A) EC50 for cell death at 96 h.
HPV negative HNSCC cell lines appear to demonstrate greater reovirus infectivity and virus-mediated oncolysis compared to HPV positive HNSCC. Reovirus shows promise as a novel therapy in HNSCC, and may be of particular benefit in HPV negative patients.
头颈部癌症晚期患者的治疗需要多学科、多模式的治疗方法,包括手术、放疗和化疗的联合应用。这些毒性治疗方案在人乳头瘤病毒(HPV)相关口咽癌的特定人群中显著改善了生存结果。HPV阴性的头颈部鳞状细胞癌(HNSCC)仍然是一个治疗挑战,因为目前的治疗方案仅使生存率有适度提高,需要创新的新治疗方法。溶瘤病毒作为低毒性辅助癌症疗法是HNSCC的新型潜在有效治疗方法。一种这样的溶瘤病毒是呼吸道孤儿肠道病毒或呼肠孤病毒。先前已证明HNSCC细胞对呼肠孤病毒感染和呼肠孤病毒诱导的细胞死亡敏感,但尚未在HPV阳性和阴性HNSCC细胞系中进行比较。
比较呼肠孤病毒在HPV阳性和阴性HNSCC细胞系中的感染性和溶瘤活性。
用系列稀释的呼肠孤病毒感染7种HNSCC细胞系。两种细胞系(UM-SCC-47和UM-SCC-104)HPV 16型呈阳性。感染18小时后,使用基于细胞的ELISA测定法测量感染性。感染96小时后,使用alamar蓝活力测定法确定溶瘤活性。使用非线性回归模型计算在50%的给定细胞系中感染和导致细胞死亡所需的病毒量(EC50)。比较EC50值。
与HPV阳性细胞系相比,HPV阴性细胞对病毒感染和溶瘤更敏感。18小时时感染性的EC50范围为感染复数(MOI)值(PFU/细胞)从18.6(SCC-9)到3133(UM-SCC 104)。96小时时细胞死亡的EC50范围为MOI(PFU/细胞)从1.02×10²(UM-SCC-14A)到3.19×10⁸(UM-SCC-47)。在96小时时,最不敏感的细胞系(UM-SCC-47)和最敏感的细胞系(UM-SCC 14A)细胞死亡的EC50之间存在3×10⁶倍的差异。
与HPV阳性HNSCC相比,HPV阴性HNSCC细胞系似乎表现出更高的呼肠孤病毒感染性和病毒介导的溶瘤作用。呼肠孤病毒作为HNSCC的一种新型疗法显示出前景,并且可能对HPV阴性患者特别有益。