Postow Michael A, Chesney Jason, Pavlick Anna C, Robert Caroline, Grossmann Kenneth, McDermott David, Linette Gerald P, Meyer Nicolas, Giguere Jeffrey K, Agarwala Sanjiv S, Shaheen Montaser, Ernstoff Marc S, Minor David, Salama April K, Taylor Matthew, Ott Patrick A, Rollin Linda M, Horak Christine, Gagnier Paul, Wolchok Jedd D, Hodi F Stephen
From Memorial Sloan Kettering Cancer Center (M.A.P., J.D.W.), Weill Cornell Medical College (M.A.P., J.D.W.), and New York University, Perlmutter Cancer Center (A.C.P.) - all in New York; J. Graham Brown Cancer Center, University of Louisville, Louisville, KY (J.C.); Institute Gustave Roussy, Villejuif (C.R.), Paris-Sud University, Orsay (C.R.), and Institut Universitaire du Cancer, Toulouse (N.M.) - all in France; Huntsman Cancer Institute, Salt Lake City (K.G.); Beth Israel Deaconess Medical Center (D. McDermott) and Dana-Farber Cancer Institute (P.A.O., F.S.H.) - both in Boston; Washington University in St. Louis, St. Louis (G.P.L.); Greenville Health System, Greenville, SC (J.K.G.); St. Luke's Cancer Center, Bethlehem, PA (S.S.A.); University of New Mexico, Albuquerque (M.S.); Taussig Cancer Institute, Cleveland Clinic Foundation, Cleveland (M.S.E.); California Pacific Center for Melanoma Research, San Francisco (D. Minor); Duke University, Durham, NC (A.K.S.); Oregon Health and Science University, Portland (M.T.); Bristol-Myers Squibb, Lawrenceville, NJ (C.H.); and Bristol-Myers Squibb, Wallingford, CT (L.M.R., P.G.).
N Engl J Med. 2015 May 21;372(21):2006-17. doi: 10.1056/NEJMoa1414428. Epub 2015 Apr 20.
In a phase 1 dose-escalation study, combined inhibition of T-cell checkpoint pathways by nivolumab and ipilimumab was associated with a high rate of objective response, including complete responses, among patients with advanced melanoma.
In this double-blind study involving 142 patients with metastatic melanoma who had not previously received treatment, we randomly assigned patients in a 2:1 ratio to receive ipilimumab (3 mg per kilogram of body weight) combined with either nivolumab (1 mg per kilogram) or placebo once every 3 weeks for four doses, followed by nivolumab (3 mg per kilogram) or placebo every 2 weeks until the occurrence of disease progression or unacceptable toxic effects. The primary end point was the rate of investigator-assessed, confirmed objective response among patients with BRAF V600 wild-type tumors.
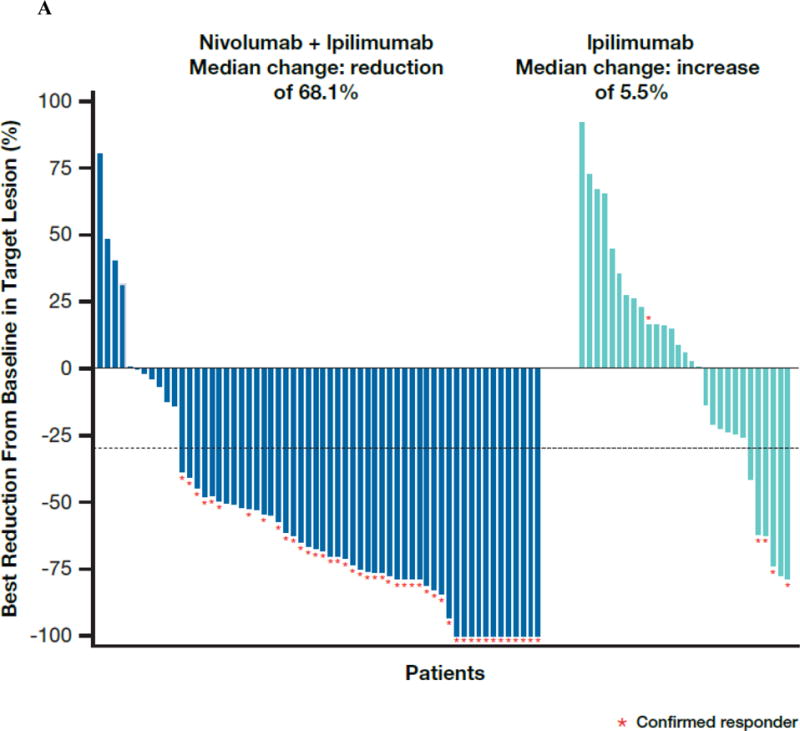
Among patients with BRAF wild-type tumors, the rate of confirmed objective response was 61% (44 of 72 patients) in the group that received both ipilimumab and nivolumab (combination group) versus 11% (4 of 37 patients) in the group that received ipilimumab and placebo (ipilimumab-monotherapy group) (P<0.001), with complete responses reported in 16 patients (22%) in the combination group and no patients in the ipilimumab-monotherapy group. The median duration of response was not reached in either group. The median progression-free survival was not reached with the combination therapy and was 4.4 months with ipilimumab monotherapy (hazard ratio associated with combination therapy as compared with ipilimumab monotherapy for disease progression or death, 0.40; 95% confidence interval, 0.23 to 0.68; P<0.001). Similar results for response rate and progression-free survival were observed in 33 patients with BRAF mutation-positive tumors. Drug-related adverse events of grade 3 or 4 were reported in 54% of the patients who received the combination therapy as compared with 24% of the patients who received ipilimumab monotherapy. Select adverse events with potential immunologic causes were consistent with those in a phase 1 study, and most of these events resolved with immune-modulating medication.
The objective-response rate and the progression-free survival among patients with advanced melanoma who had not previously received treatment were significantly greater with nivolumab combined with ipilimumab than with ipilimumab monotherapy. Combination therapy had an acceptable safety profile. (Funded by Bristol-Myers Squibb; ClinicalTrials.gov number, NCT01927419.).
在一项1期剂量递增研究中,纳武单抗和伊匹单抗联合抑制T细胞检查点通路与晚期黑色素瘤患者的高客观缓解率相关,包括完全缓解。
在这项双盲研究中,纳入了142例既往未接受过治疗的转移性黑色素瘤患者,我们以2:1的比例将患者随机分组,每3周接受一次伊匹单抗(3mg/kg体重)联合纳武单抗(1mg/kg)或安慰剂,共4剂,随后每2周接受纳武单抗(3mg/kg)或安慰剂,直至疾病进展或出现不可接受的毒性作用。主要终点是BRAF V600野生型肿瘤患者中研究者评估的、确认的客观缓解率。
在BRAF野生型肿瘤患者中,接受伊匹单抗和纳武单抗联合治疗的组(联合治疗组)确认的客观缓解率为61%(72例患者中的44例),而接受伊匹单抗和安慰剂治疗的组(伊匹单抗单药治疗组)为11%(37例患者中的4例)(P<0.001),联合治疗组有16例患者(22%)出现完全缓解,伊匹单抗单药治疗组无患者出现完全缓解。两组的中位缓解持续时间均未达到。联合治疗的中位无进展生存期未达到,伊匹单抗单药治疗的中位无进展生存期为4.4个月(联合治疗与伊匹单抗单药治疗相比,疾病进展或死亡的风险比为0.40;95%置信区间为0.23至0.68;P<0.001)。在33例BRAF突变阳性肿瘤患者中观察到了类似的缓解率和无进展生存期结果。接受联合治疗的患者中有54%报告了3级或4级药物相关不良事件,而接受伊匹单抗单药治疗的患者中这一比例为24%。具有潜在免疫原因的特定不良事件与1期研究中的事件一致,并且这些事件大多通过免疫调节药物得到缓解。
对于既往未接受过治疗的晚期黑色素瘤患者,纳武单抗联合伊匹单抗的客观缓解率和无进展生存期显著高于伊匹单抗单药治疗。联合治疗具有可接受的安全性。(由百时美施贵宝资助;ClinicalTrials.gov编号,NCT01927419。)