Fernandez-Bustamante Ana, Hashimoto Soshi, Serpa Neto Ary, Moine Pierre, Vidal Melo Marcos F, Repine John E
Department of Anesthesiology, University of Colorado SOM, Aurora, CO, USA.
Department of Anesthesiology and Webb-Waring Center, University of Colorado SOM, Aurora, CO, USA.
BMC Anesthesiol. 2015 May 6;15:56. doi: 10.1186/s12871-015-0032-x.
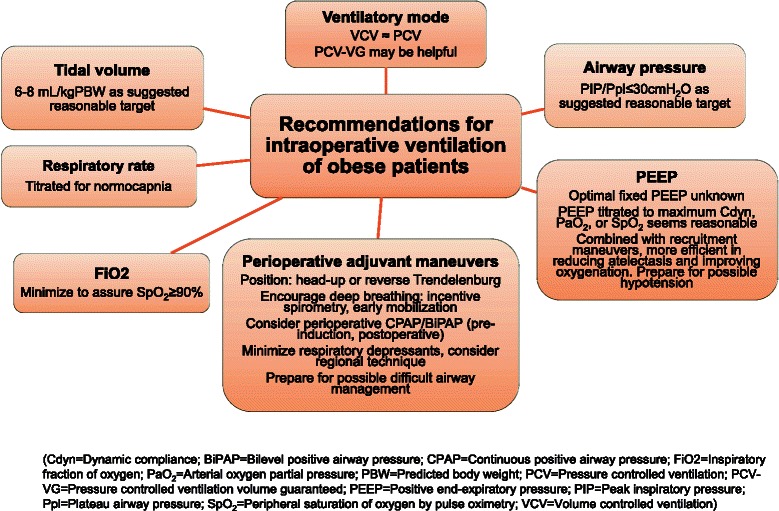
The perioperative use and relevance of protective ventilation in surgical patients is being increasingly recognized. Obesity poses particular challenges to adequate mechanical ventilation in addition to surgical constraints, primarily by restricted lung mechanics due to excessive adiposity, frequent respiratory comorbidities (i.e. sleep apnea, asthma), and concerns of postoperative respiratory depression and other pulmonary complications. The number of surgical patients with obesity is increasing, and facing these challenges is common in the operating rooms and critical care units worldwide. In this review we summarize the existing literature which supports the following recommendations for the perioperative ventilation in obese patients: (1) the use of protective ventilation with low tidal volumes (approximately 8 mL/kg, calculated based on predicted -not actual- body weight) to avoid volutrauma; (2) a focus on lung recruitment by utilizing PEEP (8-15 cmH2O) in addition to recruitment maneuvers during the intraoperative period, as well as incentivized deep breathing and noninvasive ventilation early in the postoperative period, to avoid atelectasis, hypoxemia and atelectrauma; and (3) a judicious oxygen use (ideally less than 0.8) to avoid hypoxemia but also possible reabsorption atelectasis. Obesity poses an additional challenge for achieving adequate protective ventilation during one-lung ventilation, but different lung isolation techniques have been adequately performed in obese patients by experienced providers. Postoperative efforts should be directed to avoid hypoventilation, atelectasis and hypoxemia. Further studies are needed to better define optimum protective ventilation strategies and analyze their impact on the perioperative outcomes of surgical patients with obesity.
手术患者围手术期使用保护性通气及其相关性日益受到认可。肥胖除了带来手术方面的限制外,还对充分的机械通气构成特殊挑战,主要原因包括过度肥胖导致肺力学受限、频繁的呼吸合并症(如睡眠呼吸暂停、哮喘)以及对术后呼吸抑制和其他肺部并发症的担忧。肥胖手术患者的数量在不断增加,在全球范围内的手术室和重症监护病房中,应对这些挑战很常见。在本综述中,我们总结了现有文献,这些文献支持以下针对肥胖患者围手术期通气的建议:(1)使用低潮气量(约8 mL/kg,基于预测体重而非实际体重计算)的保护性通气以避免容积伤;(2)在术中除采用肺复张手法外,利用呼气末正压通气(8 - 15 cmH₂O)关注肺复张,以及在术后早期鼓励深呼吸和无创通气,以避免肺不张、低氧血症和肺不张伤;(3)谨慎使用氧气(理想情况下小于0.8)以避免低氧血症,但也要避免可能的吸收性肺不张。肥胖对单肺通气期间实现充分的保护性通气提出了额外挑战,但经验丰富的医护人员已在肥胖患者中充分实施了不同的肺隔离技术。术后应努力避免通气不足、肺不张和低氧血症。需要进一步研究以更好地确定最佳保护性通气策略,并分析其对肥胖手术患者围手术期结局的影响。