Vermeer-de Bondt Patricia E, Schoffelen Teske, Vanrolleghem Ann M, Isken Leslie D, van Deuren Marcel, Sturkenboom Miriam C J M, Timen Aura
Centre for Infectious Disease Control, National Institute for Public Health and Environment, Bilthoven, the Netherlands.
Department of Internal Medicine, Radboud University Medical Center, Nijmegen, the Netherlands.
PLoS One. 2015 Apr 24;10(4):e0123570. doi: 10.1371/journal.pone.0123570. eCollection 2015.
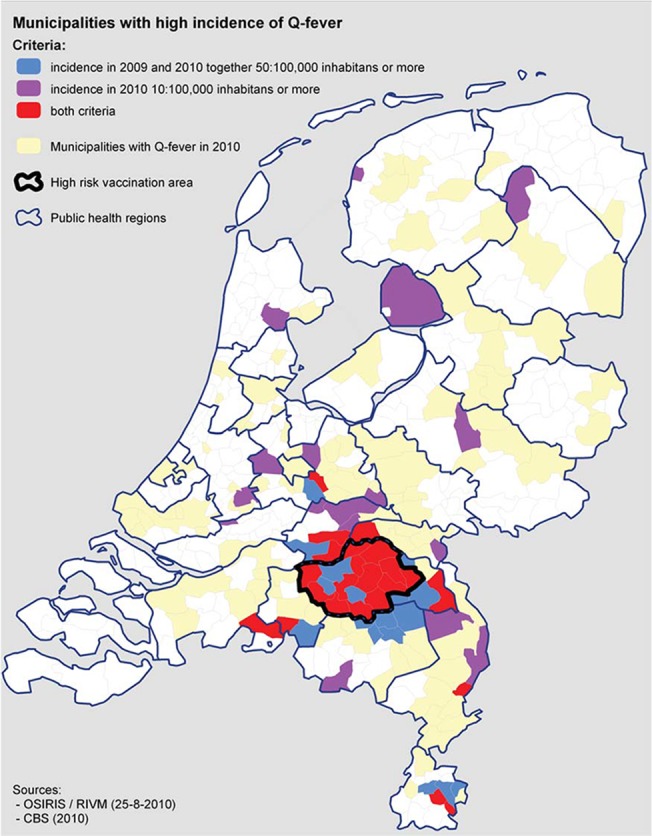
In 2011, a unique Q fever vaccination campaign targeted people at risk for chronic Q fever in the southeast of the Netherlands. General practitioners referred patients with defined cardiovascular risk-conditions (age >15 years). Prevalence rates of those risk-conditions were lacking, standing in the way of adequate planning and coverage estimation. We aimed to obtain prevalence rates retrospectively in order to estimate coverage of the Q fever vaccination campaign.
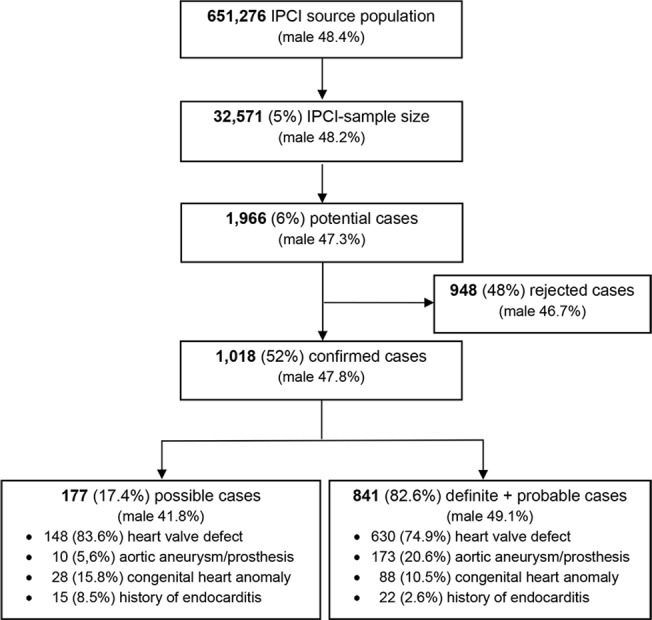
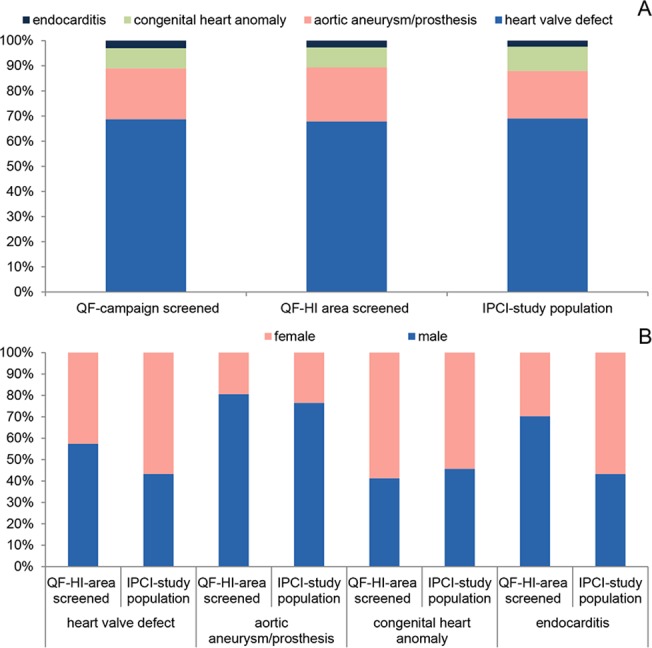
With broad search terms for these predefined risk-conditions, we extracted patient-records from a large longitudinal general-practice research-database in the Netherlands (IPCI-database). After validation of these records, obtained prevalence rates (stratified for age and sex) extrapolated to the Q fever high-incidence area population, gave an approximation of the size of the targeted patient-group. Coverage calculation addressed people actually screened by a pre-vaccination Q fever skin test and serology (coverage) and patients referred by their general practitioners (adjusted-coverage) in the 2011 campaign.
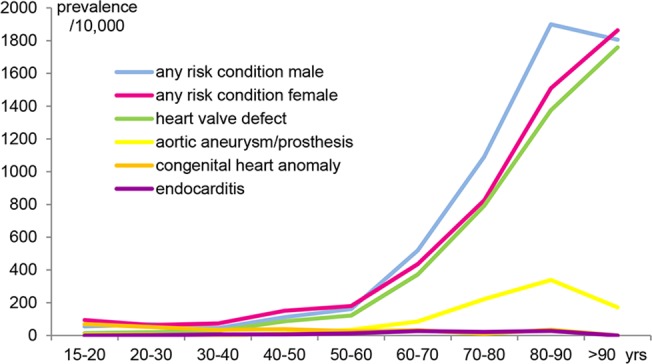
Our prevalence estimate of any risk-condition was 3.1% (lower-upper limits 2.9-3.3%). For heart valve defects, aorta aneurysm/prosthesis, congenital anomalies and endocarditis, prevalence was 2.4%, 0.6%, 0.4% and 0.1%, respectively. Estimated number of eligible people in the Q fever high-incidence area was 11,724 (10,965-12,532). With 1330 people screened for vaccination, coverage of the vaccination campaign was 11%. For referred people, the adjusted coverage was 18%. Coverage was lowest among the very-old and highest for people aged 50-70 years.
The estimated coverage of the vaccination campaign was limited. This should be interpreted in the light of the complexity of this target-group with much co-morbidity, and of the vaccine that required invasive pre-vaccination screening. Calculation of prevalence rates of risk-conditions based on the IPCI-database was feasible. This procedure proved an efficient tool for future use, when prevalence estimates for policy, implementation or surveillance of subgroup-vaccination or other health-care interventions are needed.
2011年,荷兰东南部开展了一项针对慢性Q热高危人群的独特Q热疫苗接种活动。全科医生转诊患有特定心血管风险疾病(年龄>15岁)的患者。这些风险疾病的患病率未知,这阻碍了充分的规划和覆盖率估计。我们旨在回顾性获取患病率,以估计Q热疫苗接种活动的覆盖率。
使用这些预定义风险疾病的广泛搜索词,我们从荷兰一个大型纵向全科医学研究数据库(IPCI数据库)中提取患者记录。在验证这些记录后,将获得的患病率(按年龄和性别分层)外推至Q热高发地区人群,得出目标患者群体规模的近似值。覆盖率计算涉及2011年活动中实际通过接种前Q热皮肤试验和血清学检查筛查的人群(覆盖率)以及全科医生转诊的患者(调整后覆盖率)。
我们对任何风险疾病的患病率估计为3.1%(下限-上限2.9-3.3%)。心脏瓣膜缺陷、主动脉瘤/假体、先天性异常和心内膜炎的患病率分别为2.4%、0.6%、0.4%和0.1%。Q热高发地区符合条件的人数估计为11724人(10965-12532人)。有1330人接受了疫苗接种筛查,疫苗接种活动的覆盖率为11%。对于转诊人群,调整后覆盖率为18%。覆盖率在高龄人群中最低,在50-70岁人群中最高。
疫苗接种活动的估计覆盖率有限。鉴于该目标群体合并症多的复杂性以及需要进行侵入性接种前筛查的疫苗,应这样理解这一情况。基于IPCI数据库计算风险疾病的患病率是可行的。当需要对亚组疫苗接种或其他医疗保健干预措施进行政策、实施或监测的患病率估计时,该程序被证明是一种未来可用的有效工具。