Renard Françoise, Tafforeau Jean, Deboosere Patrick
Department Public Health and Surveillance, Institute of Public Health, Brussels, Belgium.
Interface Demography, Section Social Research, Free University of Brussels, Brussels, Belgium.
Arch Public Health. 2015 Mar 23;73(1):13. doi: 10.1186/s13690-015-0060-5. eCollection 2015.
Reducing premature mortality is a crucial public health objective. The goal of this paper, beside updating previous mortality atlases with recent data, is to explore the relative between-districts disparity using a relative-scale map design.
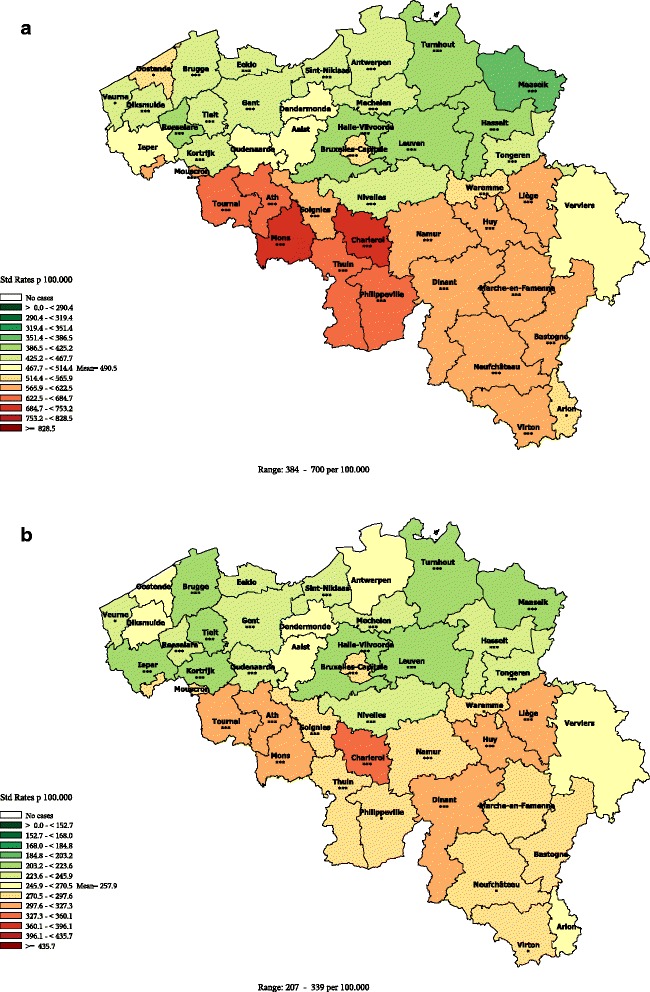
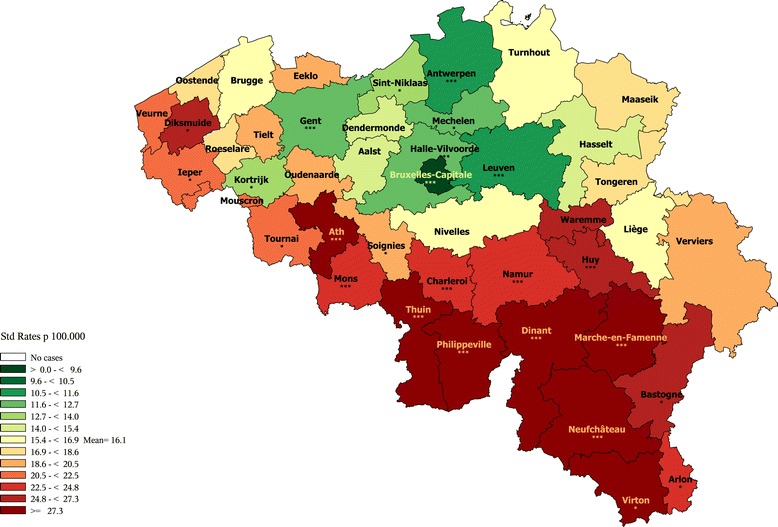
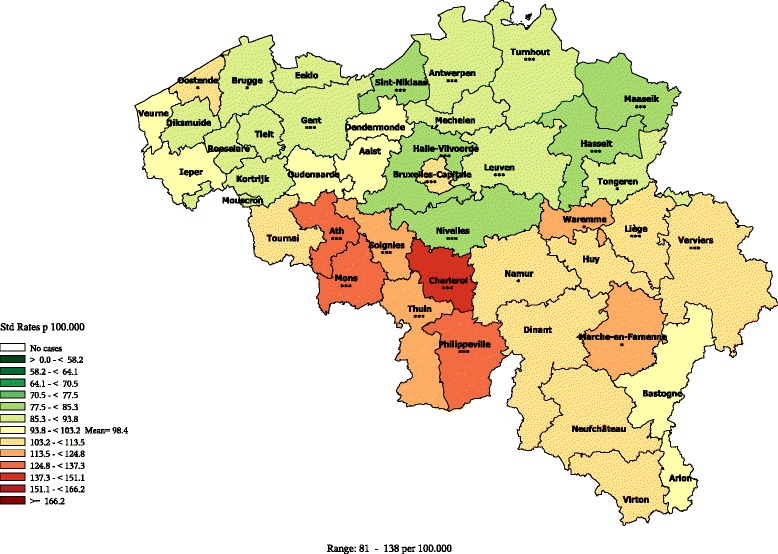
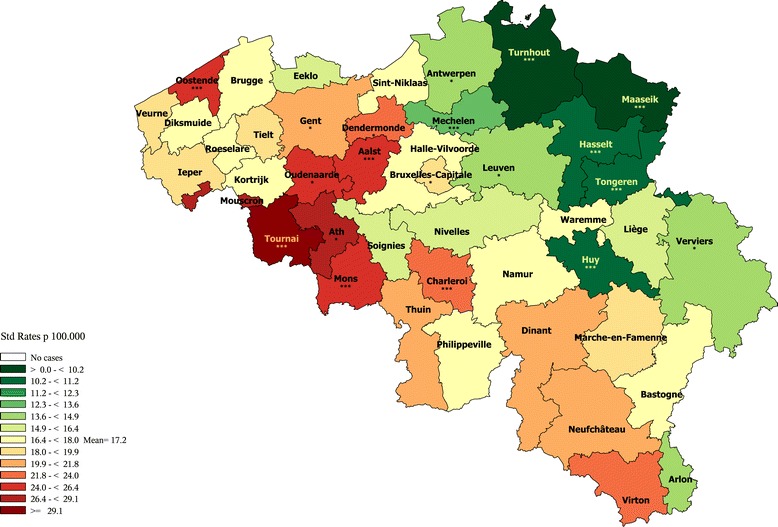
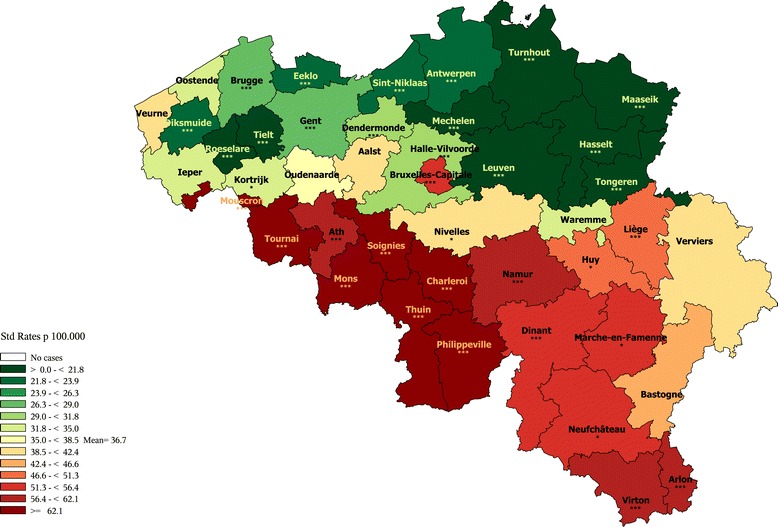
Causes of deaths and population data were provided by Statistics Belgium. All deaths occurring in the periods 1993-1999 and 2003-2009, in people aged 1-74 residing in Belgium were included. Age-adjusted rates by cause of death were computed for both periods; the 2003-2009 rates were classified using a relative scale with a 10% change between each level and represented on chloropleths maps with a green-to-red divergent colour scheme centred on the national mean. This particular design allows the comparability across all the maps since a same meaning is given to a specific colour. The variation coefficient and the decile ratio were calculated and compared between the 2 periods.
A clear-cut regional divide at the disadvantage of Wallonia, and to some extent, of Brussels, was seen for all-cause, cardiovascular, cerebrovascular, diabetes, alcohol-related, mental and neurological diseases and non-transport accidents premature mortality. A NE-SW pattern parallel to the French border was observed for Lip, Oral Cavity, Pharynx, Larynx and oesophageal cancers, while various patterns are observed for the other cancers. The highest rates of road accident mortality are observed in the Southern districts. Many of those patterns are in continuity with earlier observations. However, the pattern of diabetes and mental and neurological diseases are new features. The variation coefficient and the decile ratios increased by 10% between the 1993-1997 and 2003-2009 periods.
The use of a relative scale in the maps highlights the importance of the between-districts disparity in premature mortality, with for most causes, a clear-cut regional divide at the disadvantage of Wallonia; this health gap results of complex interactions between various factors, including the socioeconomic context, cultural habits and environmental influences, as well as public health policies. It should be considered as a warning signal, warranting the attention of the policy makers. Meanwhile, these results also highlight the potential for improvement in the more disadvantaged regions.
降低过早死亡率是一项至关重要的公共卫生目标。本文的目的,除了用最新数据更新之前的死亡率地图集外,还在于使用相对比例地图设计来探索地区间的相对差异。
死亡原因和人口数据由比利时统计局提供。纳入了1993 - 1999年和2003 - 2009年期间居住在比利时的1 - 74岁人群中的所有死亡病例。计算了两个时期按死亡原因调整的死亡率;2003 - 2009年的死亡率使用相对比例进行分类,每个级别之间有10%的变化,并在分级统计图上用以全国平均值为中心的绿到红的发散配色方案表示。这种特殊设计使得所有地图具有可比性,因为特定颜色具有相同含义。计算并比较了两个时期的变异系数和十分位数比率。
在全因、心血管、脑血管、糖尿病、酒精相关、精神和神经疾病以及非交通事故过早死亡率方面,明显存在以瓦隆地区为劣势,在一定程度上布鲁塞尔也处于劣势的区域划分。唇、口腔、咽、喉和食管癌呈现出与法国边境平行的东北 - 西南模式,而其他癌症则呈现出各种不同模式。交通事故死亡率最高的地区在南部。其中许多模式与早期观察结果一致。然而,糖尿病以及精神和神经疾病的模式是新特征。1993 - 1997年和2003 - 2009年期间,变异系数和十分位数比率增加了10%。
地图中使用相对比例突出了地区间过早死亡率差异的重要性,对于大多数死因而言,明显存在以瓦隆地区为劣势的区域划分;这种健康差距是多种因素复杂相互作用的结果,包括社会经济背景、文化习惯和环境影响以及公共卫生政策。应将其视为一个警示信号,值得政策制定者关注。同时,这些结果也凸显了较弱势地区的改善潜力。