Jiménez-Hernández Elva, Jaimes-Reyes Ethel Zulie, Arellano-Galindo José, García-Jiménez Xochiketzalli, Tiznado-García Héctor Manuel, Dueñas-González María Teresa, Martínez Villegas Octavio, Sánchez-Jara Berenice, Bekker-Méndez Vilma Carolina, Ortíz-Torres María Guadalupe, Ortíz-Fernández Antonio, Marín-Palomares Teresa, Mejía-Aranguré Juan Manuel
Departamento de Hematología Pediátrica, Unidad Médica de Alta Especialidad (UMAE), Centro Médico Nacional "La Raza", Instituto Mexicano del Seguro Social (IMSS), Avenida Jacarandas Esquina Vallejo S/N colonia La Raza, 02990 Mexico, DF, Mexico.
Laboratorio de Investigación, Hospital Infantil de México "Federico Gómez", Secretaría de Salud, Calle Doctor Marquez 162, Colonia Doctores, Delegación Cuauhtémoc, 06720 Mexico, DF, Mexico.
Biomed Res Int. 2015;2015:576950. doi: 10.1155/2015/576950. Epub 2015 Mar 26.
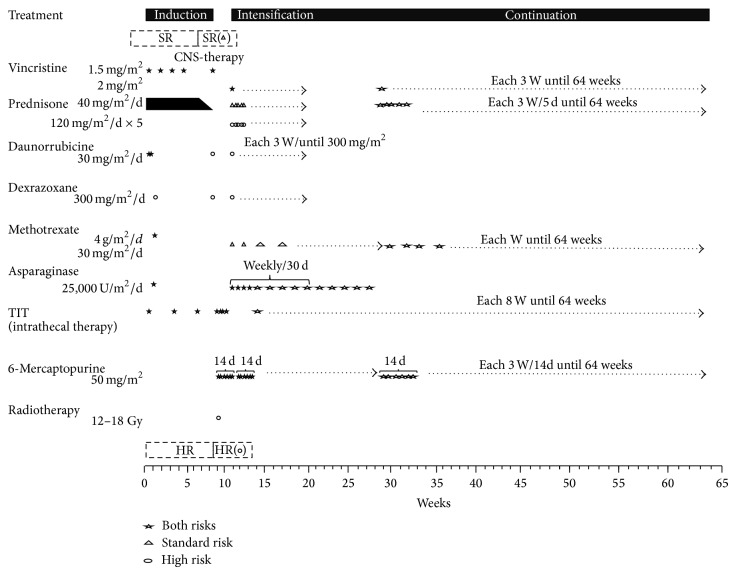
Our aim in this paper is to describe the results of treatment of acute lymphoblastic leukaemia (ALL) in Mexican children treated from 2006 to 2010 under the protocol from the Dana-Farber Cancer Institute (DFCI) 00-01. The children were younger than 16 years of age and had a diagnosis of ALL de novo. The patients were classified as standard risk if they were 1-9.9 years old and had a leucocyte count <50 × 10(9)/L, precursor B cell immunophenotype, no mediastinal mass, CSF free of blasts, and a good response to prednisone. The rest of the patients were defined as high risk. Of a total of 302 children, 51.7% were at high risk. The global survival rate was 63.9%, and the event-free survival rate was 52.3% after an average follow-up of 3.9 years. The percentages of patients who died were 7% on induction and 14.2% in complete remission; death was associated mainly with infection (21.5%). The relapse rate was 26.2%. The main factor associated with the occurrence of an event was a leucocyte count >100 × 10(9)/L. The poor outcomes were associated with toxic death during induction, complete remission, and relapse. These factors remain the main obstacles to the success of this treatment in our population.
本文的目的是描述2006年至2010年期间,按照达纳-法伯癌症研究所(DFCI)00-01方案治疗的墨西哥儿童急性淋巴细胞白血病(ALL)的治疗结果。这些儿童年龄小于16岁,初诊为ALL。如果患者年龄在1至9.9岁之间,白细胞计数<50×10⁹/L,前体B细胞免疫表型,无纵隔肿块,脑脊液无原始细胞,且对泼尼松反应良好,则被分类为标准风险。其余患者被定义为高风险。在总共302名儿童中,51.7%为高风险。平均随访3.9年后,总体生存率为63.9%,无事件生存率为52.3%。诱导期死亡患者的比例为7%,完全缓解期为14.2%;死亡主要与感染相关(21.5%)。复发率为26.2%。与事件发生相关的主要因素是白细胞计数>100×10⁹/L。不良结局与诱导期、完全缓解期和复发期的毒性死亡相关。这些因素仍然是该治疗方法在我们人群中取得成功的主要障碍。