Grodin Justin L, Mullens Wilfried, Dupont Matthias, Wu Yuping, Taylor David O, Starling Randall C, Tang W H Wilson
Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic, Cleveland, OH, USA.
Department of Cardiology, Ziekenhuis Oost-Limburg, Genk, Belgium and Hasselt University, Diepenbeek, Belgium.
Eur J Heart Fail. 2015 Jul;17(7):689-96. doi: 10.1002/ejhf.268. Epub 2015 Apr 28.
Cardiac pump function is often quantified by left ventricular ejection fraction by various imaging modalities. As the heart is commonly conceptualized as a hydraulic pump, cardiac power describes the hydraulic function of the heart. We aim to describe the prognostic value of resting cardiac power index (CPI) in ambulatory patients with advanced heart failure.
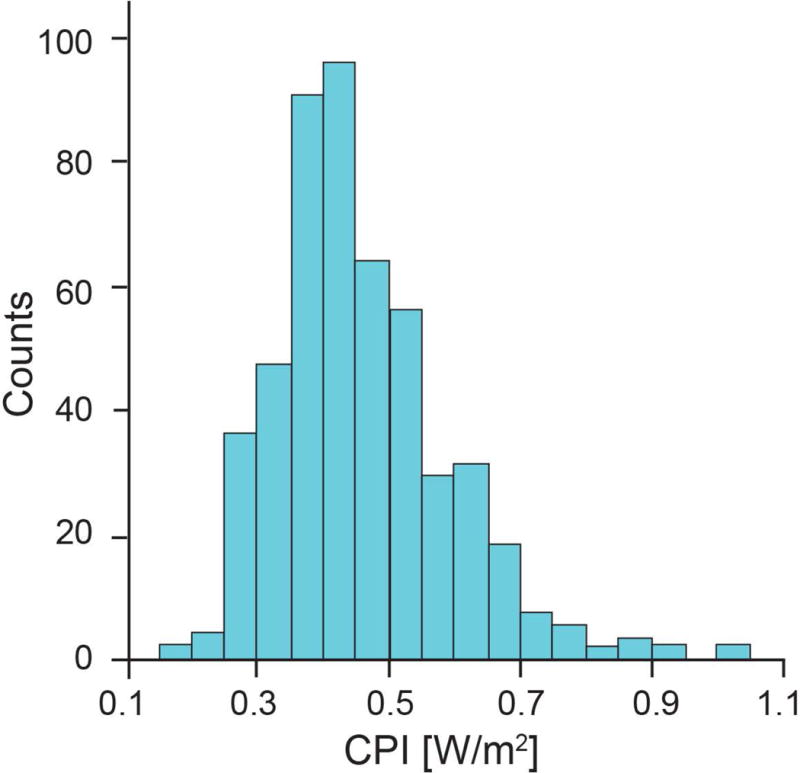
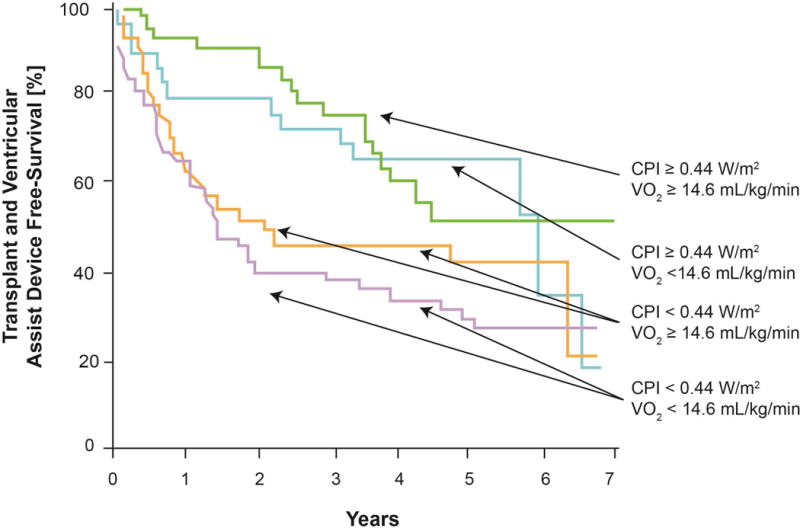
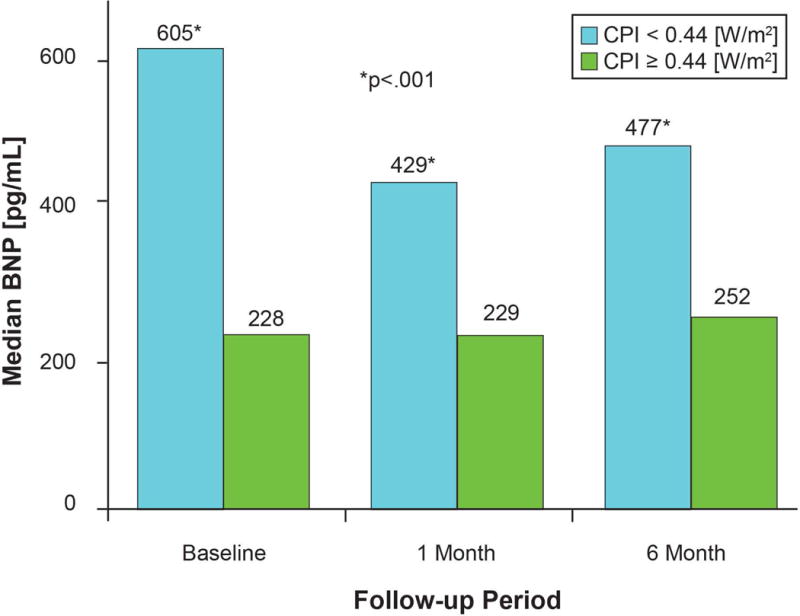
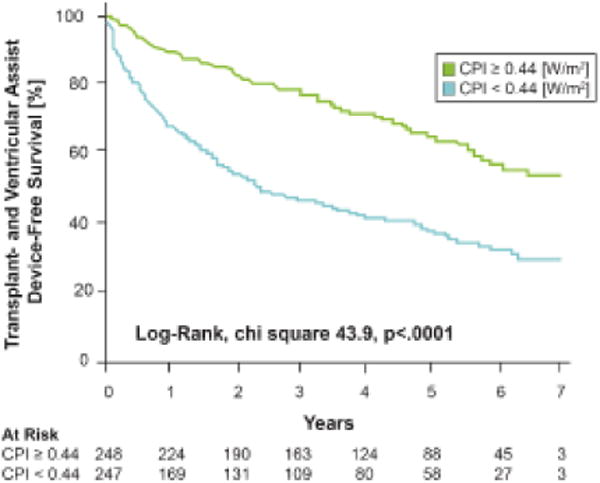
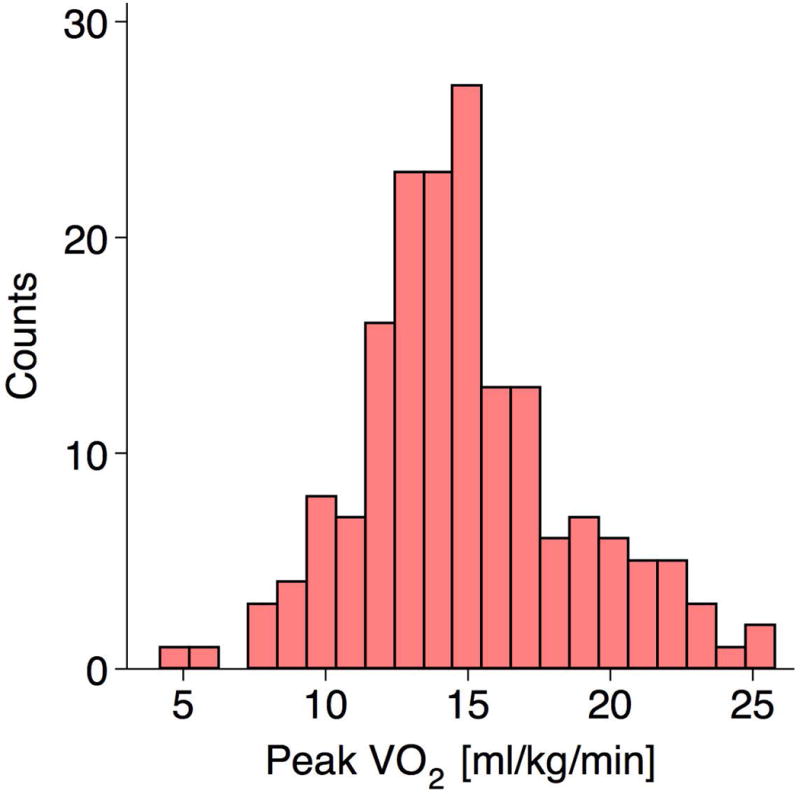
We calculated CPI in 495 sequential ambulatory patients with advanced heart failure who underwent invasive haemodynamic assessment with longitudinal follow-up of adverse outcomes (all-cause mortality, cardiac transplantation, or ventricular assist device placement). The median CPI was 0.44 W/m(2) (interquartile range 0.37, 0.52). Over a median of 3.3 years, there were 117 deaths, 104 transplants, and 20 ventricular assist device placements in our cohort. Diminished CPI (<0.44 W/m(2) ) was associated with increased adverse outcomes [hazard ratio (HR) 2.4, 95% confidence interval (CI) 1.8-3.1, P < 0.0001). The prognostic value of CPI remained significant after adjustment for age, gender, pulmonary capillary wedge pressure, cardiac index, pulmonary vascular resistance, left ventricular ejection fraction, and creatinine [HR 1.5, 95% CI 1.03-2.3, P = 0.04). Furthermore, CPI can risk stratify independently of peak oxygen consumption (HR 2.2, 95% CI 1.4-3.4, P = 0.0003).
Resting cardiac power index provides independent and incremental prediction in adverse outcomes beyond traditional haemodynamic and cardio-renal risk factors.
心脏泵功能通常通过各种成像方式的左心室射血分数来量化。由于心脏通常被视为液压泵,心脏功率描述了心脏的液压功能。我们旨在描述静息心脏功率指数(CPI)在晚期心力衰竭门诊患者中的预后价值。
我们计算了495例连续的晚期心力衰竭门诊患者的CPI,这些患者接受了有创血流动力学评估,并对不良结局(全因死亡率、心脏移植或心室辅助装置植入)进行了长期随访。CPI的中位数为0.44W/m²(四分位间距为0.37,0.52)。在我们的队列中,中位随访3.3年期间,有117例死亡、104例移植和20例心室辅助装置植入。CPI降低(<0.44W/m²)与不良结局增加相关[风险比(HR)2.4,95%置信区间(CI)1.8 - 3.1,P < 0.0001]。在对年龄、性别、肺毛细血管楔压、心脏指数、肺血管阻力、左心室射血分数和肌酐进行调整后,CPI的预后价值仍然显著[HR 1.5,95% CI 1.03 - 2.3,P = 0.04]。此外,CPI能够独立于峰值耗氧量进行风险分层(HR 2.2,95% CI 1.4 - 3.4,P = 0.0003)。
静息心脏功率指数在预测不良结局方面,能独立于传统血流动力学和心肾危险因素提供额外的预测价值。