Nielsen Anni Brit Sternhagen, Jensen Per, Gannik Dorte, Reventlow Susanne, Hollnagel Hanne, Olivarius Niels de Fine
The Research Unit for General Practice and Section of General Practice, Department of Public Health, University of Copenhagen, Copenhagen, Denmark.
Section of Biostatistics, University of Copenhagen, Copenhagen, Denmark.
BMC Public Health. 2015 Apr 30;15:439. doi: 10.1186/s12889-015-1790-6.
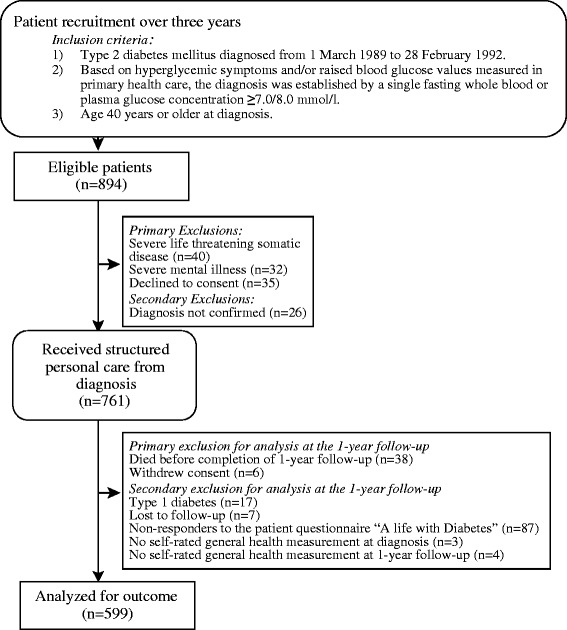
Diabetic patients' lifestyle adaptations to improve glycaemic control are not always followed by improvements in self-rated general health (SRH). The perceived impact of diabetes on patients' daily lives may influence changes in their SRH. This paper examines the association of illness severity, treatment, behavioural, and coping-related factors with changes in SRH from diagnosis of type 2 diabetes until one year later, in a population-based sample of 599 patients aged 40 years or over who were treated in general practice.
Change in SRH was estimated by a cumulative probit model with the inclusion of covariates related to SRH (e.g. illness severity at diagnosis, behaviour, treatment, and the perceived impact of diabetes on patients' daily lives one year later).
At diagnosis, 11.6% of patients reported very good, 35.1% good, 44.6% fair and 8.5% poor SRH. Physical inactivity, many diabetes-related symptoms, and cardiovascular disease were related to lower SRH ratings. On average SRH improved by 0.46 (95% CI: 0.37; 0.55) during the first year after diagnosis without inclusion of covariates. Mental and practical illness burden was the only factor associated with change in SRH, independent of patients' diabetes severity and medical treatment (p = 0.03, multivariate analysis). Compared to otherwise similar patients without illness burden, increase in SRH was marginally smaller among patients who expressed minor illness burden, but much smaller among patients with more pronounced illness burden.
Much as one would expect, many patients increased their SRH during the first year after diabetes diagnosis. This increase in SRH was not associated with indicators of illness severity or factors reflecting socio-demographic circumstances, but patients experiencing illness burden had a smaller increase than those who reported no illness burden. We suggest that during the diabetes consultation, general practitioners explore further how patients manage their illness burden. We further suggest that diabetes guidelines extend their current focus on clinical and social aspects of diabetes to include questions on patient's perceived illness burden and SRH.
糖尿病患者为改善血糖控制而进行的生活方式调整,并不总能带来自评总体健康状况(SRH)的改善。糖尿病对患者日常生活的感知影响可能会影响其SRH的变化。本文在一个基于人群的样本中,研究了599名年龄在40岁及以上、在全科医疗中接受治疗的患者,从2型糖尿病诊断到一年后SRH变化与疾病严重程度、治疗、行为及应对相关因素之间的关联。
通过累积概率模型估计SRH的变化,并纳入与SRH相关的协变量(如诊断时的疾病严重程度、行为、治疗以及一年后糖尿病对患者日常生活的感知影响)。
诊断时,11.6%的患者报告SRH非常好,35.1%的患者报告良好,44.6%的患者报告一般,8.5%的患者报告较差。缺乏身体活动、许多糖尿病相关症状以及心血管疾病与较低的SRH评分相关。在不纳入协变量的情况下,诊断后的第一年SRH平均改善了0.46(95%置信区间:0.37;0.55)。心理和实际疾病负担是与SRH变化相关的唯一因素,独立于患者的糖尿病严重程度和医疗治疗(多变量分析,p = 0.03)。与其他情况相似但无疾病负担的患者相比,有轻微疾病负担的患者SRH的增加略小,而疾病负担更明显的患者SRH的增加则小得多。
正如人们所预期的那样,许多患者在糖尿病诊断后的第一年提高了他们的SRH。SRH的这种增加与疾病严重程度指标或反映社会人口统计学情况的因素无关,但有疾病负担的患者的增加幅度小于那些报告无疾病负担的患者。我们建议在糖尿病咨询过程中,全科医生进一步探讨患者如何应对他们的疾病负担。我们还建议糖尿病指南将目前对糖尿病临床和社会方面的关注扩展到包括患者感知的疾病负担和SRH相关问题。