Charytan David M, Lewis Eldrin F, Desai Akshay S, Weinrauch Larry A, Ivanovich Peter, Toto Robert D, Claggett Brian, Liu Jiankang, Hartley L Howard, Finn Peter, Singh Ajay K, Levey Andrew S, Pfeffer Marc A, McMurray John J V, Solomon Scott D
Renal Division, Department of Medicine, Brigham & Women's Hospital, Boston, MA.
Cardiovascular Division, Department of Medicine, Brigham & Women's Hospital, Boston, MA.
Am J Kidney Dis. 2015 Sep;66(3):429-40. doi: 10.1053/j.ajkd.2015.02.324. Epub 2015 Apr 29.
The cause of death in patients with chronic kidney disease (CKD) varies with CKD severity, but variation has not been quantified.
Retrospective analysis of prospective randomized clinical trial.
SETTING & PARTICIPANTS: We analyzed 4,038 individuals with anemia and diabetic CKD from TREAT, a randomized trial comparing darbepoetin alfa and placebo.
Baseline estimated glomerular filtration rate (eGFR) and protein-creatinine ratio (PCR).
Cause of death as adjudicated by a blinded committee.
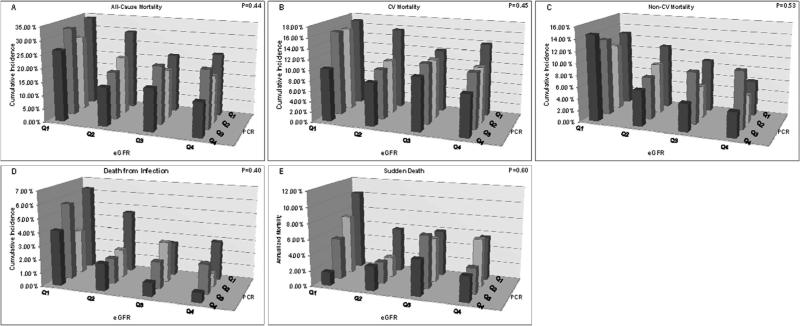
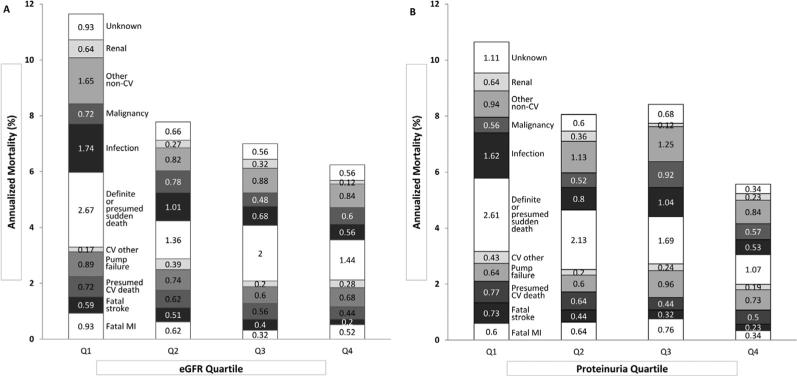
Median eGFR and PCR ranged from 20.6 mL/min/1.73 m(2) and 4.1 g/g in quartile 1 (Q1) to 47.0 mL/min/1.73 m(2) and 0.1 g/g in Q4 (P<0.01). Of 806 deaths, 441, 298, and 67 were due to cardiovascular (CV), non-CV, and unknown causes, respectively. Cumulative CV mortality at 3 years was higher with lower eGFR (Q1, 15.5%; Q2, 11.1%; Q3, 11.2%; Q4, 10.3%; P<0.001) or higher PCR (Q1, 15.2%; Q2, 12.3%; Q3, 11.7%; Q4, 9.0%; P<0.001). Similarly, non-CV mortality was higher with lower eGFR (Q1, 12.7%; Q2, 8.4%; Q3, 6.7%; Q4, 6.1%; P<0.001) or higher PCR (Q1, 10.3%; Q2, 7.9%; Q3, 9.4%; Q4, 6.4%; P=0.01). Sudden death was 1.7-fold higher with lower eGFR (P=0.04) and 2.1-fold higher with higher PCR (P<0.001). Infection-related mortality was 3.3-fold higher in the lowest eGFR quartile (P<0.001) and 2.8-fold higher in the highest PCR quartile (P<0.02). The overall proportion of CV and non-CV deaths was not significantly different across eGFR or PCR quartiles.
Results may not be generalizable to nondiabetic CKD or diabetic CKD in the absence of anemia. Measured GFR was not available.
In diabetic CKD, both lower baseline GFR and higher PCR are associated with higher CV and non-CV mortality rates, particularly from sudden death and infection. Efforts to improve outcomes should focus on CV disease and early diagnosis and treatment of infection.
慢性肾脏病(CKD)患者的死因随CKD严重程度而异,但这种差异尚未被量化。
对前瞻性随机临床试验进行回顾性分析。
我们分析了来自TREAT研究的4038例贫血和糖尿病性CKD患者,该研究是一项比较达比加群酯和安慰剂的随机试验。
基线估计肾小球滤过率(eGFR)和蛋白肌酐比值(PCR)。
由盲法委员会判定的死因。
eGFR和PCR的中位数在第1四分位数(Q1)中为20.6 mL/min/1.73 m²和4.1 g/g,在第4四分位数(Q4)中为47.0 mL/min/1.73 m²和0.1 g/g(P<0.01)。在806例死亡病例中,分别有441例、298例和67例死于心血管(CV)、非CV和不明原因。3年时,eGFR较低(Q1,15.5%;Q2,11.1%;Q3,11.2%;Q4,10.3%;P<0.001)或PCR较高(Q1,15.2%;Q2,12.3%;Q3,11.7%;Q4,9.0%;P<0.001)时,累积CV死亡率较高。同样,eGFR较低(Q1,12.7%;Q2,8.4%;Q3,6.7%;Q4,6.1%;P<0.001)或PCR较高(Q1,10.3%;Q2,7.9%;Q3,9.4%;Q4,6.4%;P=0.01)时,非CV死亡率较高。eGFR较低时猝死率高1.7倍(P=0.04);PCR较高时猝死率高2.1倍(P<0.001)。最低eGFR四分位数组的感染相关死亡率高3.3倍(P<0.001),最高PCR四分位数组的感染相关死亡率高2.8倍(P<0.02)。不同eGFR或PCR四分位数组中CV和非CV死亡的总体比例无显著差异。
结果可能不适用于非糖尿病性CKD或无贫血的糖尿病性CKD。无法获得测量的GFR。
在糖尿病性CKD中,较低的基线GFR和较高的PCR均与较高的CV和非CV死亡率相关,尤其是猝死和感染导致的死亡率。改善预后的努力应侧重于心血管疾病以及感染的早期诊断和治疗。