Wagih Alaa, Mohsen Laila, Rayan Moustafa M, Hasan Mo'men M, Al-Sherif Ashraf H
Department of Radiology, Minia University, Minia, Egypt.
Department of Obstetrics and Gynecology, Minia University, Minia, Egypt.
Pol J Radiol. 2015 Apr 25;80:210-6. doi: 10.12659/PJR.893460. eCollection 2015.
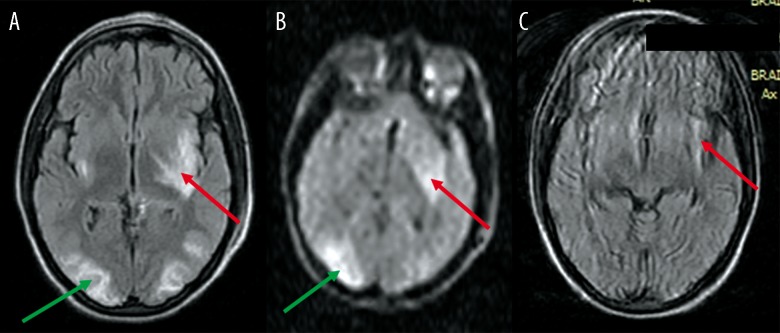
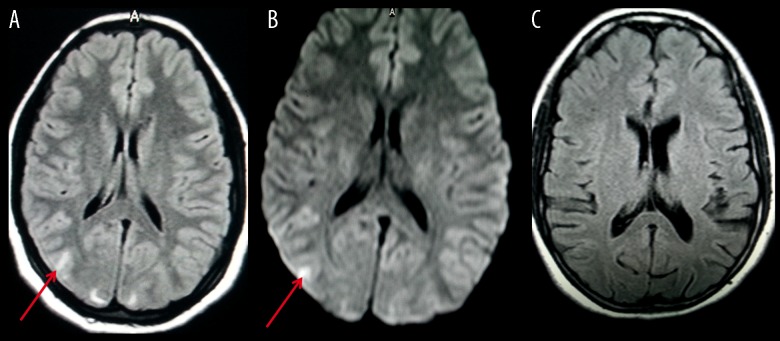
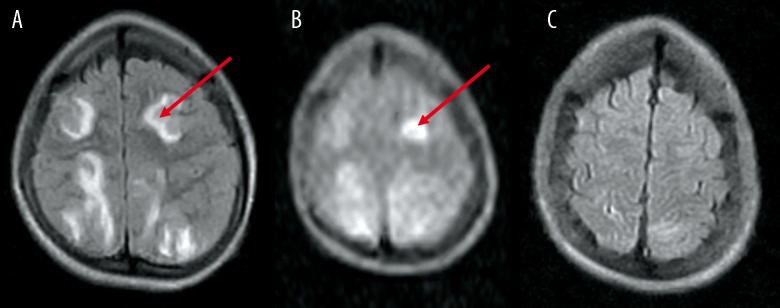
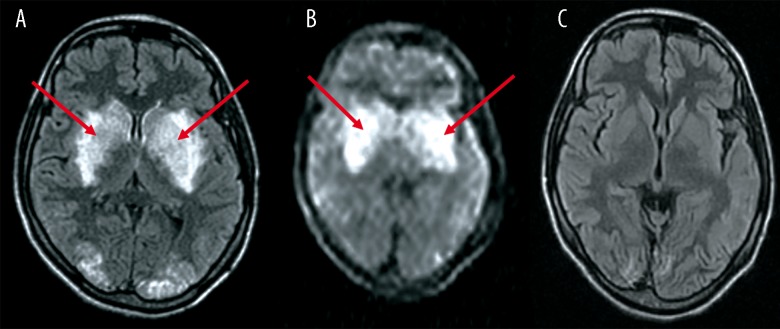
Restricted diffusion is the second most common atypical presentation of PRES. This has a very important implication, as lesions with cytotoxic edema may progress to infarction. Several studies suggested the role of DWI in the prediction of development of infarctions in these cases. Other studies, however, suggested that PRES is reversible even with cytotoxic patterns. Our aim was to evaluate whether every restricted diffusion in PRES is reversible and what factors affect this reversibility.
MATERIAL/METHODS: Thirty-six patients with acute neurological symptoms suggestive of PRES were included in our study. Inclusion criteria comprised imaging features of atypical PRES where DWI images and ADC maps show restricted diffusion. Patients were imaged with 0.2-T and 1.5-T machines. FLAIR images were evaluated for the severity of the disease and a FLAIR/DWI score was used. ADC values were selectively recorded from the areas of diffusion restriction. A follow-up MRI study was carried out in all patients after 2 weeks. Patients were classified according to reversibility into: Group 1 (reversible PRES; 32 patients) and Group 2 (irreversible changes; 4 patients). The study was approved by the University's research ethics committee, which conforms to the declaration of Helsinki.
The age and blood pressure did not vary significantly between both groups. The total number of regions involved and the FLAIR/DWI score did not vary significantly between both groups. Individual regions did not reveal any tendency for the development of irreversible lesions. Similarly, ADC values did not reveal any significant difference between both groups.
PRES is completely reversible in the majority of patients, even with restricted diffusion. None of the variables under study could predict the reversibility of PRES lesions. It seems that this process is individual-dependent.
扩散受限是 PRES 第二常见的非典型表现。这具有非常重要的意义,因为伴有细胞毒性水肿的病变可能进展为梗死。多项研究提示 DWI 在预测这些病例梗死发展中的作用。然而,其他研究表明即使存在细胞毒性模式,PRES 也是可逆的。我们的目的是评估 PRES 中所有的扩散受限是否都可逆以及哪些因素影响这种可逆性。
材料/方法:我们的研究纳入了 36 例有提示 PRES 的急性神经症状的患者。纳入标准包括非典型 PRES 的影像学特征,即 DWI 图像和 ADC 图显示扩散受限。患者使用 0.2-T 和 1.5-T 机器进行成像。评估 FLAIR 图像以确定疾病严重程度,并使用 FLAIR/DWI 评分。从扩散受限区域选择性记录 ADC 值。所有患者在 2 周后进行了随访 MRI 研究。根据可逆性将患者分为:第 1 组(可逆性 PRES;32 例患者)和第 2 组(不可逆性改变;4 例患者)。该研究得到了大学研究伦理委员会的批准,该委员会符合赫尔辛基宣言。
两组之间的年龄和血压无显著差异。两组之间受累区域总数和 FLAIR/DWI 评分无显著差异。各个区域未显示出不可逆病变发展的任何趋势。同样,两组之间的 ADC 值也未显示出任何显著差异。
即使存在扩散受限,大多数患者的 PRES 也是完全可逆的。所研究的变量均无法预测 PRES 病变的可逆性。似乎这个过程是个体依赖的。