Rono Josea, Färnert Anna, Murungi Linda, Ojal John, Kamuyu Gathoni, Guleid Fatuma, Nyangweso George, Wambua Juliana, Kitsao Barnes, Olotu Ally, Marsh Kevin, Osier Faith Ha
KEMRI-Wellcome Trust Research Programme, Centre for Geographical Medicine Research-Coast, Kilifi, Kenya.
Infectious Diseases Unit, Department of Medicine, Solna, Karolinska Institutet, Stockholm, Sweden.
BMC Med. 2015 May 13;13:114. doi: 10.1186/s12916-015-0354-z.
Epidemiological studies indicate that some children experience many more episodes of clinical malaria than their age mates in a given location. Whether this is as a result of the micro-heterogeneity of malaria transmission with some children effectively getting more exposure to infectious mosquitoes than others, or reflects a failure in the acquisition of immunity needs to be elucidated. Here, we investigated the determinants of increased susceptibility to clinical malaria by comparing the intensity of exposure to Plasmodium falciparum and the acquisition of immunity in children at the extreme ends of the over-dispersed distribution of the incidence of clinical malaria.
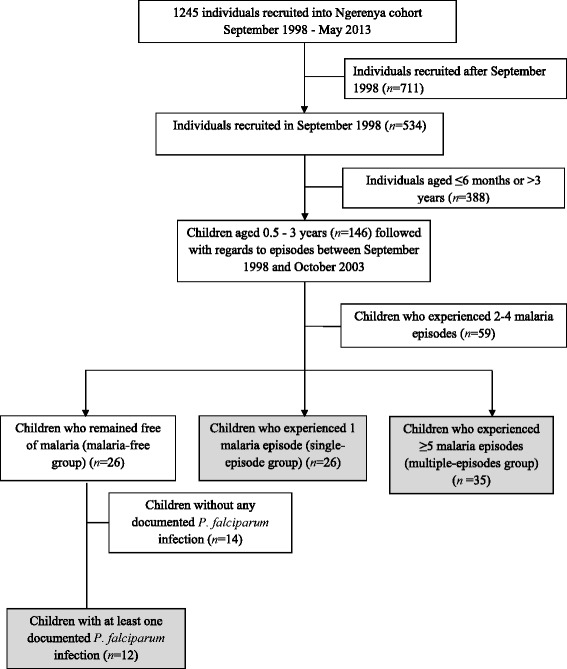
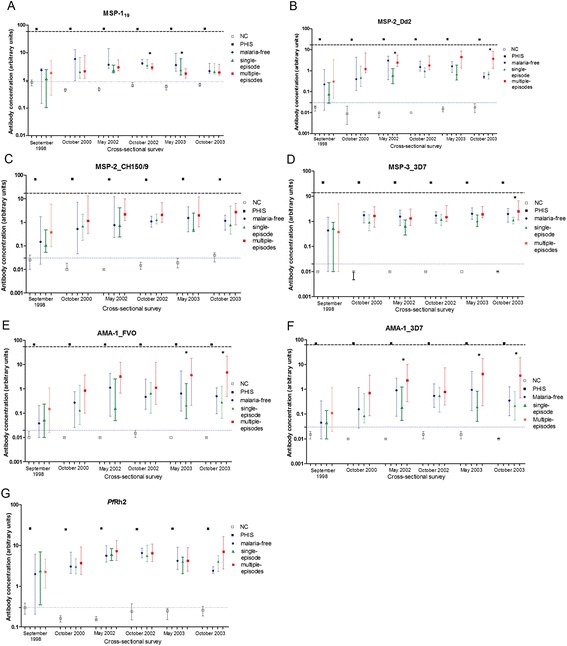
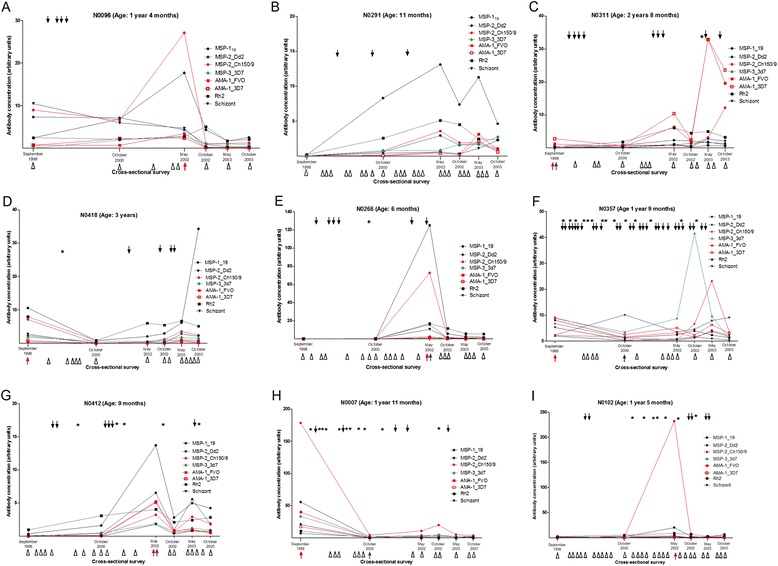
The study was nested within a larger cohort in an area where the intensity of malaria transmission was low. We identified children who over a five-year period experienced 5 to 16 clinical malaria episodes (children at the tail-end of the over-dispersed distribution, n = 35), remained malaria-free (n = 12) or had a single episode (n = 26). We quantified antibodies against seven Plasmodium falciparum merozoite antigens in plasma obtained at six cross-sectional surveys spanning these five years. We analyzed the antibody responses to identify temporal dynamics that associate with disease susceptibility.
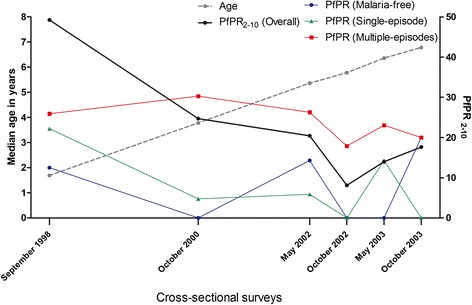
Children experiencing multiple episodes of malaria were more likely to be parasite positive by microscopy at cross-sectional surveys (X (2) test for trend 14.72 P = 0.001) and had a significantly higher malaria exposure index, than those in the malaria-free or single episode groups (Kruskal-Wallis test P = 0.009). In contrast, the five-year temporal dynamics of anti-merozoite antibodies were similar in the three groups. Importantly in all groups, antibody levels were below the threshold concentrations previously observed to be correlated with protective immunity.
We conclude that in the context of a low malaria transmission setting, susceptibility to clinical malaria is not accounted for by anti-merozoite antibodies but appears to be a consequence of increased parasite exposure. We hypothesize that intensive exposure is a prerequisite for protective antibody concentrations, while little to modest exposure may manifest as multiple clinical infections with low levels of antibodies. These findings have implications for interventions that effectively lower malaria transmission intensity.
流行病学研究表明,在特定地区,一些儿童经历的临床疟疾发作次数比同龄人多得多。这是由于疟疾传播的微观异质性,导致一些儿童比其他儿童更易接触到感染性蚊子,还是反映出免疫获得失败,尚需阐明。在此,我们通过比较临床疟疾发病率过度分散分布两端儿童对恶性疟原虫的暴露强度和免疫获得情况,研究了临床疟疾易感性增加的决定因素。
该研究嵌套于疟疾传播强度较低地区的一个更大队列中。我们确定了在五年期间经历5至16次临床疟疾发作的儿童(处于过度分散分布尾端的儿童,n = 35)、未患疟疾的儿童(n = 12)或仅有一次发作的儿童(n = 26)。我们在这五年期间的六次横断面调查中,对血浆中针对七种恶性疟原虫裂殖子抗原的抗体进行了定量。我们分析了抗体反应,以确定与疾病易感性相关的时间动态变化。
在横断面调查中,经历多次疟疾发作的儿童通过显微镜检查更可能呈寄生虫阳性(趋势X(2)检验,14.72,P = 0.001),且疟疾暴露指数显著高于未患疟疾或仅有一次发作的儿童组(Kruskal-Wallis检验,P = 0.009)。相比之下,三组中抗裂殖子抗体的五年时间动态变化相似。重要的是,在所有组中,抗体水平均低于先前观察到的与保护性免疫相关的阈值浓度。
我们得出结论,在疟疾传播率较低的环境中,临床疟疾易感性并非由抗裂殖子抗体所致,而似乎是寄生虫暴露增加的结果。我们推测,高强度暴露是产生保护性抗体浓度的先决条件,而低至适度暴露可能表现为多次临床感染且抗体水平较低。这些发现对有效降低疟疾传播强度的干预措施具有启示意义。