Arya Supreeta, Das Deepak, Engineer Reena, Saklani Avanish
Department of Radio-Diagnosis, Tata Memorial Centre, Mumbai, Maharashtra, India.
Department of Radiation Oncology, Tata Memorial Centre, Mumbai, Maharashtra, India.
Indian J Radiol Imaging. 2015 Apr-Jun;25(2):148-61. doi: 10.4103/0971-3026.155865.
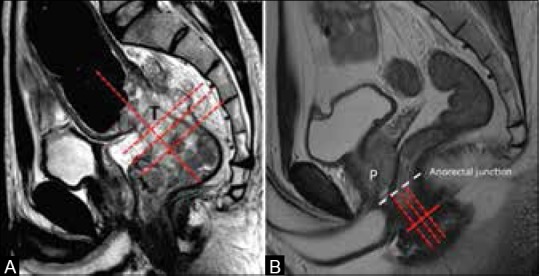
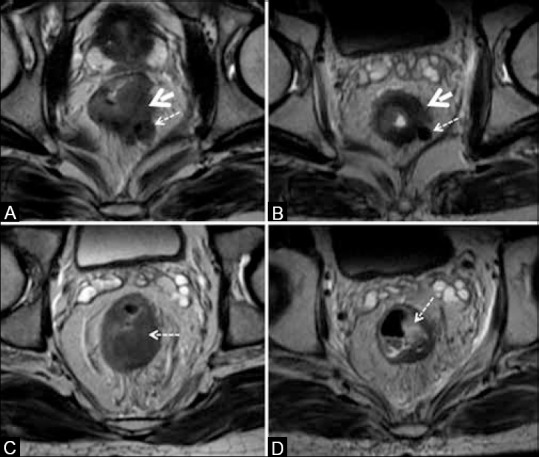
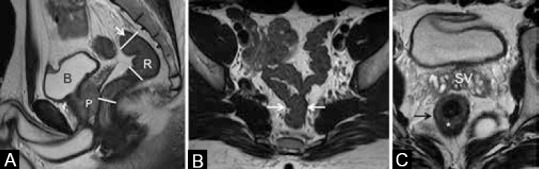
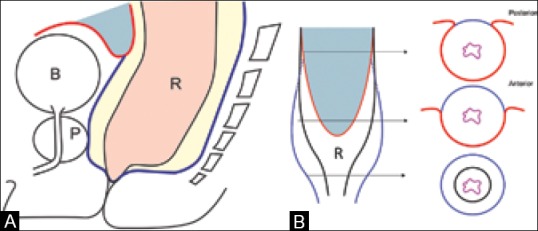
Imaging in rectal cancer has a vital role in staging disease, and in selecting and optimizing treatment planning. High-resolution MRI (HR-MRI) is the recommended method of first choice for local staging of rectal cancer for both primary staging and for restaging after preoperative chemoradiation (CT-RT). HR-MRI helps decide between upfront surgery and preoperative CT-RT. It provides high accuracy for prediction of circumferential resection margin at surgery, T category, and nodal status in that order. MRI also helps assess resectability after preoperative CT-RT and decide between sphincter saving or more radical surgery. Accurate technique is crucial for obtaining high-resolution images in the appropriate planes for correct staging. The phased array external coil has replaced the endorectal coil that is no longer recommended. Non-fat suppressed 2D T2-weighted (T2W) sequences in orthogonal planes to the tumor are sufficient for primary staging. Contrast-enhanced MRI is considered inappropriate for both primary staging and restaging. Diffusion-weighted sequence may be of value in restaging. Multidetector CT cannot replace MRI in local staging, but has an important role for evaluating distant metastases. Positron emission tomography-computed tomography (PET/CT) has a limited role in the initial staging of rectal cancer and is reserved for cases with resectable metastatic disease before contemplating surgery. This article briefly reviews the comprehensive role of imaging in rectal cancer, describes the role of MRI in local staging in detail, discusses the optimal MRI technique, and provides a synoptic report for both primary staging and restaging after CT-RT in routine practice.
直肠癌的影像学检查在疾病分期、治疗方案的选择及优化方面发挥着至关重要的作用。高分辨率磁共振成像(HR - MRI)是直肠癌局部分期的首选推荐方法,无论是用于初始分期还是术前放化疗(CT - RT)后的再分期。HR - MRI有助于在直接手术和术前CT - RT之间做出决策。它依次对手术切缘、T分期及淋巴结状态的预测具有较高准确性。MRI还可用于评估术前CT - RT后的可切除性,并决定是保留括约肌还是采取更根治性的手术。准确的技术对于在合适的平面获取高分辨率图像以进行正确分期至关重要。相控阵体表线圈已取代了不再推荐使用的直肠内线圈。与肿瘤呈正交平面的非脂肪抑制二维T2加权(T2W)序列足以进行初始分期。对比增强MRI对于初始分期和再分期均不适用。扩散加权序列在再分期中可能有价值。多排CT在局部分期中无法替代MRI,但在评估远处转移方面具有重要作用。正电子发射断层扫描 - 计算机断层扫描(PET/CT)在直肠癌的初始分期中作用有限,仅适用于考虑手术前可切除转移性疾病的病例。本文简要回顾了影像学检查在直肠癌中的综合作用,详细描述了MRI在局部分期中的作用,讨论了最佳MRI技术,并提供了常规实践中CT - RT后初始分期和再分期的简要报告。