Pena Michelle J, Heinzel Andreas, Heinze Georg, Alkhalaf Alaa, Bakker Stephan J L, Nguyen Tri Q, Goldschmeding Roel, Bilo Henk J G, Perco Paul, Mayer Bernd, de Zeeuw Dick, Lambers Heerspink Hiddo J
Department of Clinical Pharmacy & Pharmacology, University of Groningen, University Medical Center Groningen, Groningen, The Netherlands.
emergentec biodevelopment GmbH, Vienna, Austria.
PLoS One. 2015 May 14;10(5):e0120995. doi: 10.1371/journal.pone.0120995. eCollection 2015.
We aimed to identify a novel panel of biomarkers predicting renal function decline in type 2 diabetes, using biomarkers representing different disease pathways speculated to contribute to the progression of diabetic nephropathy.
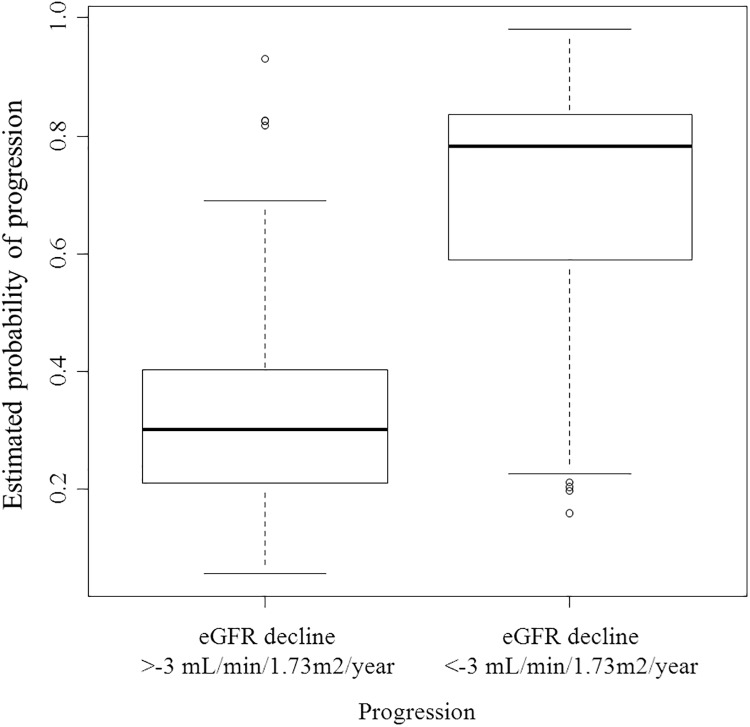
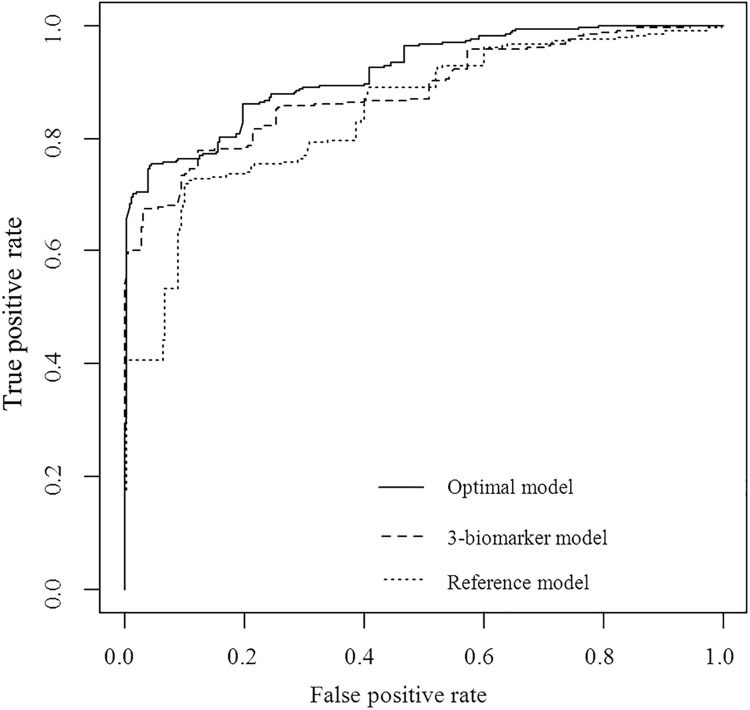
A systematic data integration approach was used to select biomarkers representing different disease pathways. Twenty-eight biomarkers were measured in 82 patients seen at an outpatient diabetes center in The Netherlands. Median follow-up was 4.0 years. We compared the cross-validated explained variation (R2) of two models to predict eGFR decline, one including only established risk markers, the other adding a novel panel of biomarkers. Least absolute shrinkage and selection operator (LASSO) was used for model estimation. The C-index was calculated to assess improvement in prediction of accelerated eGFR decline defined as <-3.0 mL/min/1.73m2/year.
Patients' average age was 63.5 years and baseline eGFR was 77.9 mL/min/1.73m2. The average rate of eGFR decline was -2.0 ± 4.7 mL/min/1.73m2/year. When modeled on top of established risk markers, the biomarker panel including matrix metallopeptidases, tyrosine kinase, podocin, CTGF, TNF-receptor-1, sclerostin, CCL2, YKL-40, and NT-proCNP improved the explained variability of eGFR decline (R2 increase from 37.7% to 54.6%; p=0.018) and improved prediction of accelerated eGFR decline (C-index increase from 0.835 to 0.896; p=0.008).
A novel panel of biomarkers representing different pathways of renal disease progression including inflammation, fibrosis, angiogenesis, and endothelial function improved prediction of eGFR decline on top of established risk markers in type 2 diabetes. These results need to be confirmed in a large prospective cohort.
我们旨在利用代表推测与糖尿病肾病进展相关的不同疾病途径的生物标志物,确定一组预测2型糖尿病肾功能下降的新型生物标志物。
采用系统的数据整合方法选择代表不同疾病途径的生物标志物。在荷兰一家门诊糖尿病中心就诊的82例患者中测量了28种生物标志物。中位随访时间为4.0年。我们比较了两个预测估算肾小球滤过率(eGFR)下降模型的交叉验证解释变异(R2),一个模型仅包括已确定的风险标志物,另一个模型增加了一组新型生物标志物。使用最小绝对收缩和选择算子(LASSO)进行模型估计。计算C指数以评估对定义为<-3.0 mL/min/1.73m2/年的加速eGFR下降预测的改善情况。
患者的平均年龄为63.5岁,基线eGFR为77.9 mL/min/1.73m2。eGFR下降的平均速率为-2.0±4.7 mL/min/1.73m2/年。在已确定的风险标志物基础上进行建模时,包括基质金属肽酶、酪氨酸激酶、足突蛋白、结缔组织生长因子、肿瘤坏死因子受体-1、硬化蛋白、趋化因子配体2、YKL-40和N末端前脑钠肽(NT-proCNP)的生物标志物组改善了eGFR下降的解释变异性(R2从37.7%增加到54.6%;p=0.018),并改善了对加速eGFR下降的预测(C指数从0.835增加到0.896;p=0.008)。
一组代表肾脏疾病进展不同途径(包括炎症、纤维化、血管生成和内皮功能)的新型生物标志物,在已确定的2型糖尿病风险标志物基础上改善了对eGFR下降的预测。这些结果需要在大型前瞻性队列中得到证实。