Trachet Bram, Fraga-Silva Rodrigo A, Londono Francisco J, Swillens Abigaïl, Stergiopulos Nikolaos, Segers Patrick
IBiTech-bioMMeda, Ghent University-IMinds Medical IT, Ghent, Belgium; Institute of Bioengineering, Ecole Polytechnique Federale de Lausanne, Lausanne, Switzerland.
Institute of Bioengineering, Ecole Polytechnique Federale de Lausanne, Lausanne, Switzerland.
PLoS One. 2015 May 29;10(5):e0129007. doi: 10.1371/journal.pone.0129007. eCollection 2015.
Several ultrasound-based methods are currently used to assess aortic diameter, circumferential strain and stiffness in mice, but none of them is flawless and a gold standard is lacking. We aimed to assess the validity and sensitivity of these methods in control animals and animals developing dissecting abdominal aortic aneurysm.
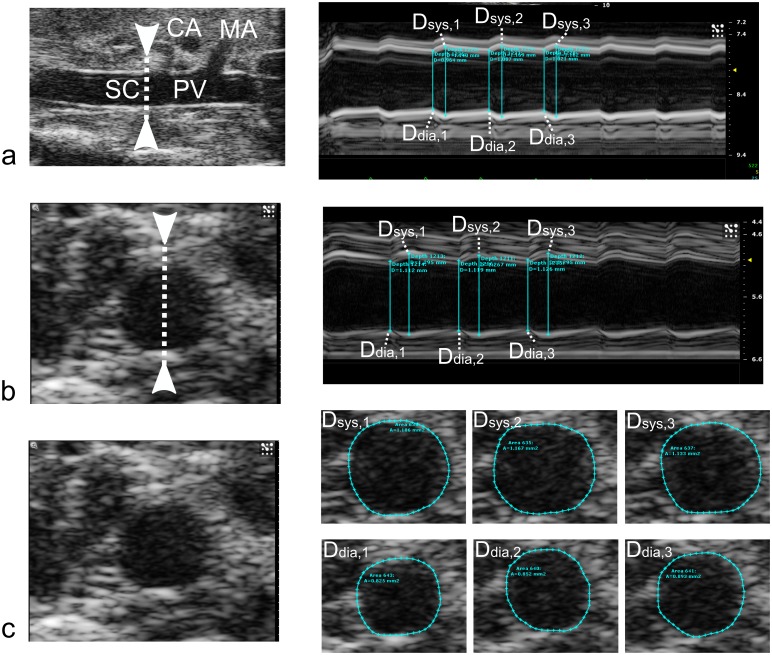
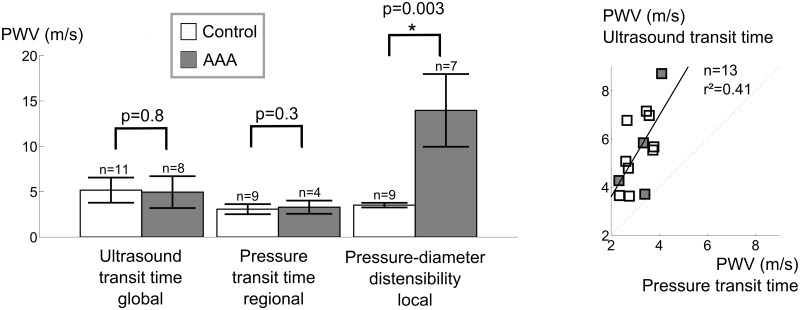
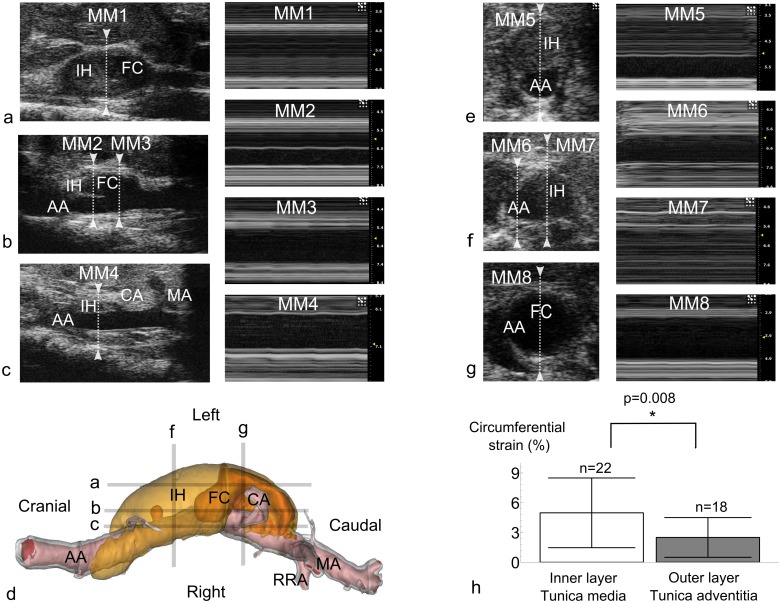
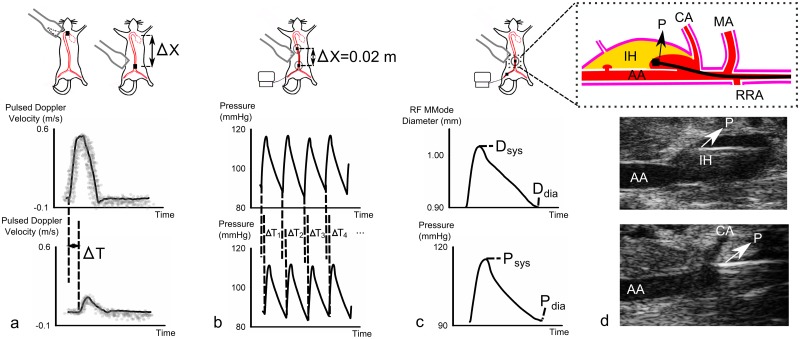
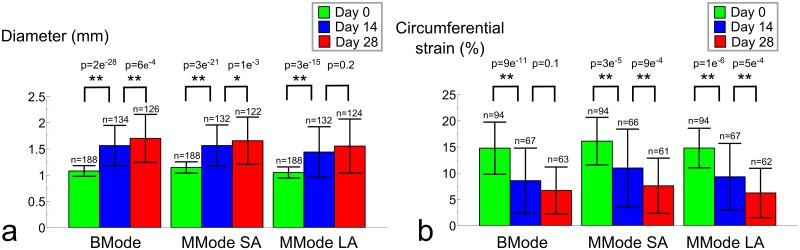
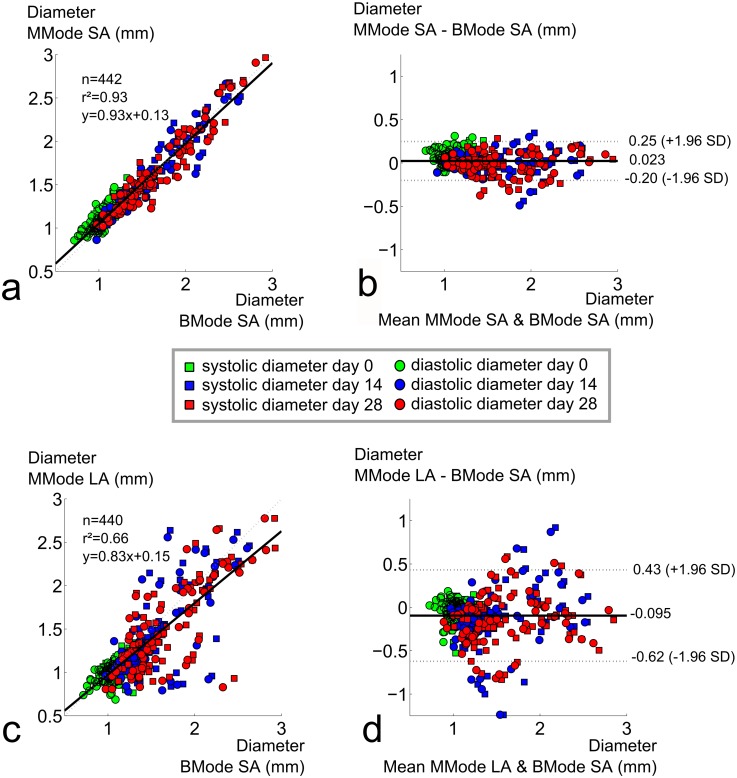
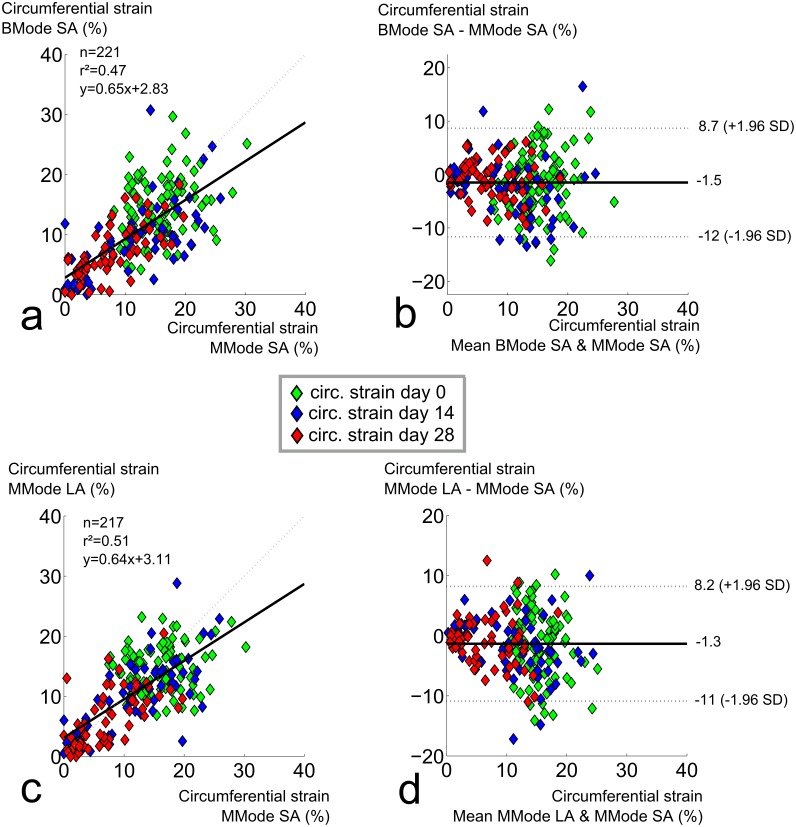
We first compared systolic and diastolic diameters as well as local circumferential strains obtained in 47 Angiotensin II-infused ApoE(-/-) mice with three different techniques (BMode, short axis MMode, long axis MMode), at two different abdominal aortic locations (supraceliac and paravisceral), and at three different time points of abdominal aneurysm formation (baseline, 14 days and 28 days). We found that short axis BMode was preferred to assess diameters, but should be avoided for strains. Short axis MMode gave good results for diameters but high standard deviations for strains. Long axis MMode should be avoided for diameters, and was comparable to short axis MMode for strains. We then compared pulse wave velocity measurements using global, ultrasound-based transit time or regional, pressure-based transit time in 10 control and 20 angiotensin II-infused, anti-TGF-Beta injected C57BL/6 mice. Both transit-time methods poorly correlated and were not able to detect a significant difference in PWV between controls and aneurysms. However, a combination of invasive pressure and MMode diameter, based on radio-frequency data, detected a highly significant difference in local aortic stiffness between controls and aneurysms, with low standard deviation.
In small animal ultrasound the short axis view is preferred over the long axis view to measure aortic diameters, local methods are preferred over transit-time methods to measure aortic stiffness, invasive pressure-diameter data are preferred over non-invasive strains to measure local aortic stiffness, and the use of radiofrequency data improves the accuracy of diameter, strain as well as stiffness measurements.
目前有几种基于超声的方法用于评估小鼠的主动脉直径、圆周应变和僵硬度,但这些方法都并非完美无缺,且缺乏金标准。我们旨在评估这些方法在对照动物和发生腹主动脉夹层动脉瘤的动物中的有效性和敏感性。
我们首先比较了通过三种不同技术(B 型模式、短轴 M 型模式、长轴 M 型模式)在 47 只接受血管紧张素 II 注射的 ApoE(-/-)小鼠的两个不同腹主动脉位置(腹腔干上方和内脏旁)以及腹主动脉瘤形成的三个不同时间点(基线、14 天和 28 天)所获得的收缩期和舒张期直径以及局部圆周应变。我们发现短轴 B 型模式更适合评估直径,但不适合用于应变评估。短轴 M 型模式在直径评估方面效果良好,但应变的标准差较高。长轴 M 型模式不适合用于直径评估,在应变评估方面与短轴 M 型模式相当。然后我们比较了 10 只对照小鼠和 20 只接受血管紧张素 II 注射并注射抗转化生长因子-β的 C57BL/6 小鼠中使用基于超声的整体传输时间或基于压力的局部传输时间进行的脉搏波速度测量。两种传输时间方法的相关性都很差,并且无法检测到对照组和动脉瘤组之间脉搏波速度的显著差异。然而,基于射频数据的有创压力和 M 型模式直径的组合检测到对照组和动脉瘤组之间局部主动脉僵硬度存在高度显著差异,且标准差较低。
在小动物超声检查中,测量主动脉直径时短轴视图优于长轴视图,测量主动脉僵硬度时局部方法优于传输时间方法,测量局部主动脉僵硬度时基于有创压力 - 直径的数据优于无创应变数据,并且使用射频数据可提高直径、应变以及僵硬度测量的准确性。