Iqbal Javaid, Serruys Patrick W, Silber Sigmund, Kelbaek Henning, Richardt Gert, Morel Marie-Angele, Negoita Manuela, Buszman Pawel E, Windecker Stephan
From the Department of Interventional Cardiology, Erasmus Medical Centre, Rotterdam, The Netherlands (J.I., P.W.S.); Department of Cardiovascular Science, University of Sheffield, UK (J.I.); International Centre for Circulatory Health, Imperial College London, London, UK (P.W.S.); Department of Cardiology, Heart Centre at the Isar, Munich, Germany (S.S.); Righshospitalet, The Heart Center, Copenhagen, Denmark (H.K.); Herzzentrum der Segeberger Kliniken, Bad Segeberg, Germany (G.R.); Cardialysis BV, Rotterdam, The Netherlands (M.-A.M.); Medtronic, Santa Rosa, CA (M.N.); Department of Cardiology, Medical University of Silesia, Katowice, Poland (P.E.B.); and Department of Cardiology, Bern University Hospital, Bern, Switzerland (S.W.).
Circ Cardiovasc Interv. 2015 Jun;8(6):e002230. doi: 10.1161/CIRCINTERVENTIONS.114.002230.
Newer-generation drug-eluting stents that release zotarolimus or everolimus have been shown to be superior to the first-generation drug-eluting stents. However, data comparing long-term safety and efficacy of zotarolimus- (ZES) and everolimus-eluting stents (EES) are limited. RESOLUTE all-comers (Randomized Comparison of a Zotarolimus-Eluting Stent With an Everolimus-Eluting Stent for Percutaneous Coronary Intervention) trial compared these 2 stents and has shown that ZES was noninferior to EES at 12-month for the primary end point of target lesion failure. We report the secondary clinical outcomes at the final 5-year follow-up of this trial.
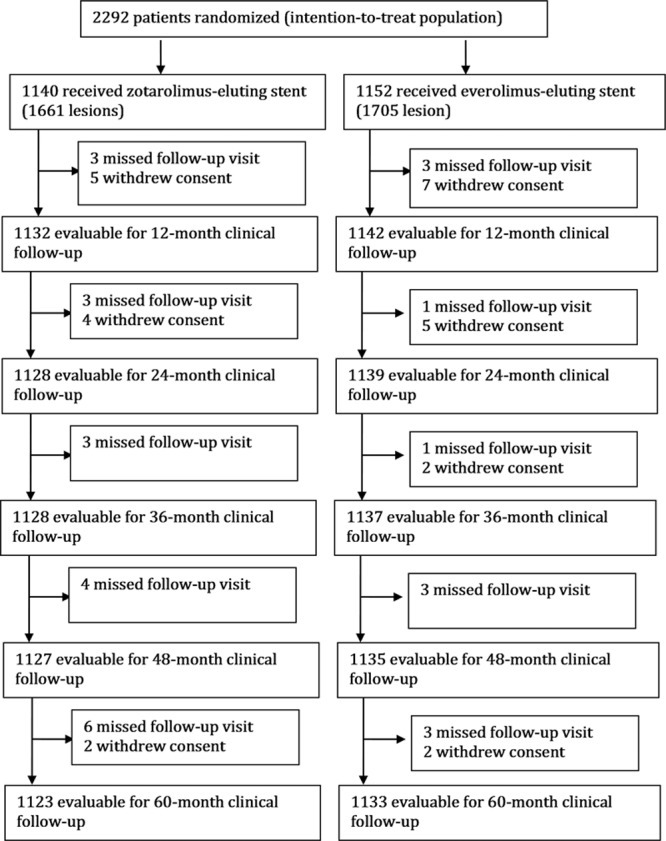
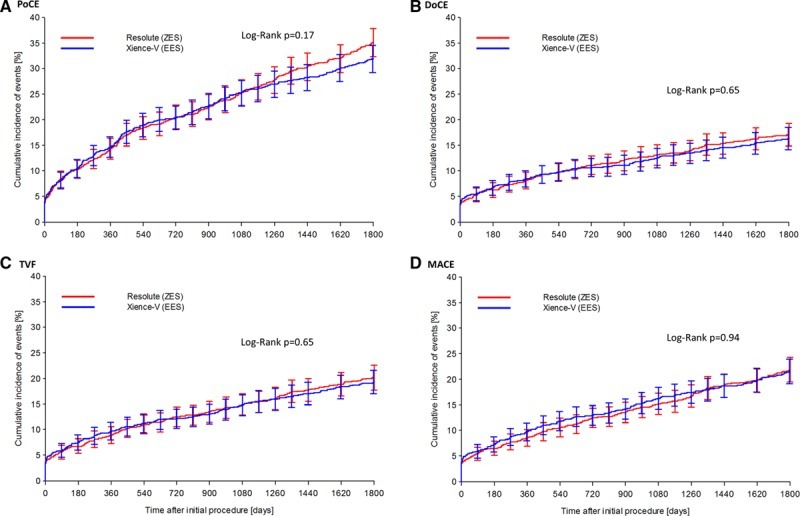
RESOLUTE all-comer clinical study is a prospective, multicentre, randomized, 2-arm, open-label, noninferiority trial with minimal exclusion criteria. Patients (n=2292) were randomly assigned to treatment with either ZES (n=1140) or EES (n=1152). Patient-oriented composite end point (combination of all-cause mortality, myocardial infarction, and any revascularizations), device-oriented composite end point (combination of cardiac death, target vessel myocardial infarction, and clinically indicated target lesion revascularization), and major adverse cardiac events (combination of all-cause death, all myocardial infarction, emergent coronary bypass surgery, or clinically indicated target lesion revascularization) were analyzed at 5-year follow-up. The 2 groups were well-matched at baseline. Five-year follow-up data were available for 98% patients. There were no differences in patient-oriented composite end point (ZES 35.3% versus EES 32.0%, P=0.11), device-oriented composite end point (ZES 17.0% versus EES 16.2%, P=0.61), major adverse cardiac events (ZES 21.9% versus EES 21.6%, P=0.88), and definite/probable stent thrombosis (ZES 2.8% versus EES 1.8%, P=0.12).
At 5-year follow-up, ZES and EES had similar efficacy and safety in a population of patients who had minimal exclusion criteria.
URL: http://www.clinicaltrials.gov. Unique identifier: NCT00617084.
已证实新一代释放佐他莫司或依维莫司的药物洗脱支架优于第一代药物洗脱支架。然而,比较佐他莫司洗脱支架(ZES)和依维莫司洗脱支架(EES)长期安全性和有效性的数据有限。RESOLUTE全人群试验(一项比较佐他莫司洗脱支架与依维莫司洗脱支架用于经皮冠状动脉介入治疗的随机对照试验)对这两种支架进行了比较,并表明在12个月时,ZES在靶病变失败的主要终点方面不劣于EES。我们报告了该试验最终5年随访时的次要临床结局。
RESOLUTE全人群临床研究是一项前瞻性、多中心、随机、双臂、开放标签、非劣效性试验,排除标准极少。患者(n = 2292)被随机分配接受ZES(n = 1140)或EES(n = 1152)治疗。在5年随访时分析了以患者为导向的复合终点(全因死亡、心肌梗死和任何血管重建的组合)、以器械为导向的复合终点(心源性死亡、靶血管心肌梗死和临床指征的靶病变血管重建的组合)以及主要不良心脏事件(全因死亡、所有心肌梗死、急诊冠状动脉搭桥手术或临床指征的靶病变血管重建的组合)。两组在基线时匹配良好。98%的患者有5年随访数据。在以患者为导向的复合终点方面(ZES为35.3%,EES为32.0%,P = 0.11)、以器械为导向的复合终点方面(ZES为17.0%,EES为16.2%,P = 0.61)、主要不良心脏事件方面(ZES为21.9%,EES为21.6%,P = 0.88)以及明确/可能的支架血栓形成方面(ZES为2.8%,EES为1.8%,P = 0.12)均无差异。
在5年随访时,对于排除标准极少的患者群体,ZES和EES具有相似的疗效和安全性。