Piette John D, Striplin Dana, Marinec Nicolle, Chen Jenny, Trivedi Ranak B, Aron David C, Fisher Lawrence, Aikens James E
Center for Clinical Management Research and Center for Managing Chronic Disease, VA Ann Arbor Healthcare System and University of Michigan School of Public Health, Ann Arbor, MI, United States.
J Med Internet Res. 2015 Jun 10;17(6):e142. doi: 10.2196/jmir.4550.
Mobile health (mHealth) interventions may improve heart failure (HF) self-care, but standard models do not address informal caregivers' needs for information about the patient's status or how the caregiver can help.
We evaluated mHealth support for caregivers of HF patients over and above the impact of a standard mHealth approach.
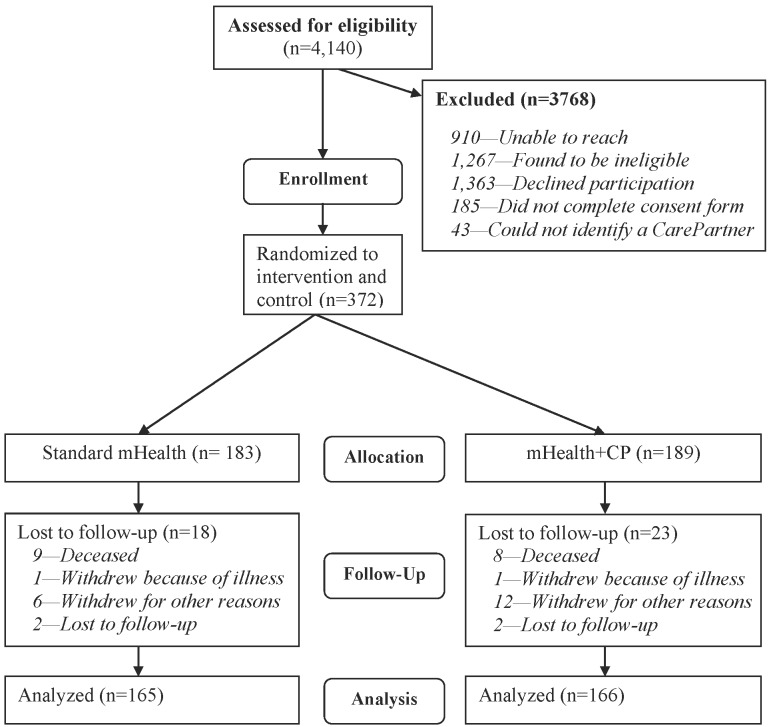
We identified 331 HF patients from Department of Veterans Affairs outpatient clinics. All patients identified a "CarePartner" outside their household. Patients randomized to "standard mHealth" (n=165) received 12 months of weekly interactive voice response (IVR) calls including questions about their health and self-management. Based on patients' responses, they received tailored self-management advice, and their clinical team received structured fax alerts regarding serious health concerns. Patients randomized to "mHealth+CP" (n=166) received an identical intervention, but with automated emails sent to their CarePartner after each IVR call, including feedback about the patient's status and suggestions for how the CarePartner could support disease care. Self-care and symptoms were measured via 6- and 12-month telephone surveys with a research associate. Self-care and symptom data also were collected through the weekly IVR assessments.
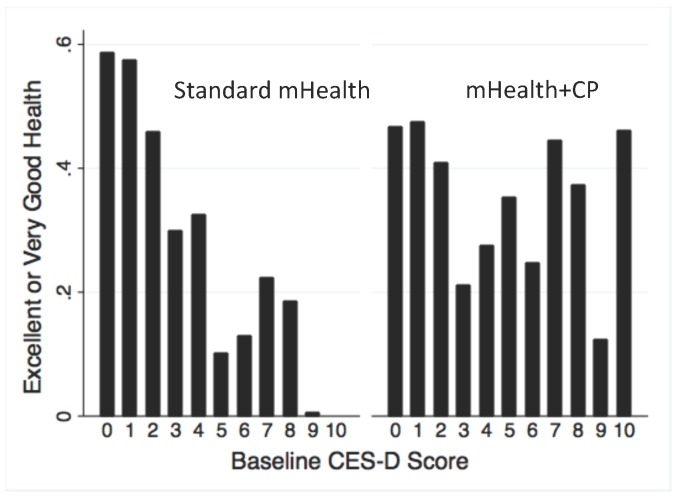
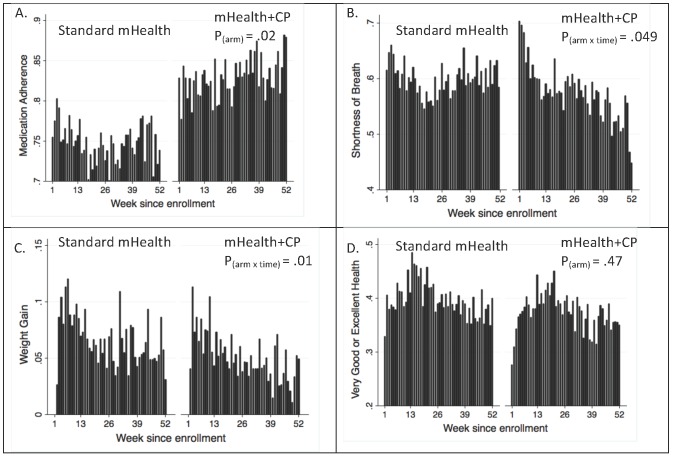
Participants were on average 67.8 years of age, 99% were male (329/331), 77% where white (255/331), and 59% were married (195/331). During 15,709 call-weeks of attempted IVR assessments, patients completed 90% of their calls with no difference in completion rates between arms. At both endpoints, composite quality of life scores were similar across arms. However, more mHealth+CP patients reported taking medications as prescribed at 6 months (8.8% more, 95% CI 1.2-16.5, P=.02) and 12 months (13.8% more, CI 3.7-23.8, P<.01), and 10.2% more mHealth+CP patients reported talking with their CarePartner at least twice per week at the 6-month follow-up (P=.048). mHealth+CP patients were less likely to report negative emotions during those interactions at both endpoints (both P<.05), were consistently more likely to report taking medications as prescribed during weekly IVR assessments, and also were less likely to report breathing problems or weight gains (all P<.05). Among patients with more depressive symptoms at enrollment, those randomized to mHealth+CP were more likely than standard mHealth patients to report excellent or very good general health during weekly IVR calls.
Compared to a relatively intensive model of IVR monitoring, self-management assistance, and clinician alerts, a model including automated feedback to an informal caregiver outside the household improved HF patients' medication adherence and caregiver communication. mHealth+CP may also decrease patients' risk of HF exacerbations related to shortness of breath and sudden weight gains. mHealth+CP may improve quality of life among patients with greater depressive symptoms. Weekly health and self-care monitoring via mHealth tools may identify intervention effects in mHealth trials that go undetected using typical, infrequent retrospective surveys.
ClinicalTrials.gov NCT00555360; https://clinicaltrials.gov/ct2/show/NCT00555360 (Archived by WebCite at http://www.webcitation.org/6Z4Tsk78B).

移动健康(mHealth)干预可能会改善心力衰竭(HF)的自我护理,但标准模式并未满足非正式护理人员了解患者状况或如何提供帮助的信息需求。
我们评估了mHealth对HF患者护理人员的支持作用,以及其相对于标准mHealth方法的额外影响。
我们从退伍军人事务部门诊诊所识别出331名HF患者。所有患者均指定了一名家庭以外的“护理伙伴”。随机分配至“标准mHealth”组(n = 165)的患者接受为期12个月的每周交互式语音应答(IVR)电话,内容包括关于他们的健康和自我管理的问题。根据患者的回答,他们会收到量身定制的自我管理建议,其临床团队会收到关于严重健康问题的结构化传真警报。随机分配至“mHealth + CP”组(n = 166)的患者接受相同的干预,但每次IVR电话后会自动向其护理伙伴发送电子邮件,包括患者状况的反馈以及护理伙伴如何支持疾病护理的建议。通过与研究助理进行的6个月和12个月电话调查来测量自我护理和症状。自我护理和症状数据也通过每周的IVR评估收集。
参与者的平均年龄为67.8岁,99%为男性(329/331),77%为白人(255/331),59%已婚(195/331)。在15,709个尝试进行IVR评估的呼叫周期间,患者完成了90%的呼叫,两组的完成率无差异。在两个终点,各治疗组的综合生活质量评分相似。然而,更多的mHealth + CP组患者在6个月时报告按规定服药(多8.8%,95%CI 1.2 - 16.5,P = 0.02)和12个月时(多13.8%,CI 3.7 - 23.8,P < 0.01),并且在6个月随访时,mHealth + CP组患者中多10.2%报告每周至少与护理伙伴交谈两次(P = 0.048)。在两个终点,mHealth + CP组患者在这些互动中报告负面情绪的可能性较小(均P < 0.05),在每周IVR评估期间持续更有可能报告按规定服药,并且报告呼吸问题或体重增加的可能性也较小(均P < 0.05)。在入组时抑郁症状较多的患者中,随机分配至mHealth + CP组的患者比标准mHealth组患者在每周IVR电话中更有可能报告总体健康状况为优秀或非常好。
与相对密集的IVR监测、自我管理协助和临床医生警报模式相比,一种包括向家庭以外的非正式护理人员提供自动反馈的模式改善了HF患者的药物依从性和护理人员沟通。mHealth + CP还可能降低患者因呼吸急促和体重突然增加导致HF恶化的风险。mHealth + CP可能改善抑郁症状较重患者的生活质量。通过mHealth工具进行的每周健康和自我护理监测可能会识别出mHealth试验中的干预效果,而这些效果使用典型的、不频繁的回顾性调查可能无法检测到。
ClinicalTrials.gov NCT00555360;https://clinicaltrials.gov/ct2/show/NCT00555360(由WebCite存档于http://www.webcitation.org/6Z4Tsk78B)。